

Keep your distance!
Distance and demarcation as forms of protective spatial planning against plague and cholera in Venice, Vienna and Hamburg
By art historian Jens Niebaum
“pro inspiratione diuina quodammodo ordinatus”: the lazaretto in Venice
When the plague struck Venice once again in 1423, the Senate decided to set up a new type of hospital to house and care for all infected people from Venice and its islands, a small island off the Lido on which the monastery of Santa Maria di Nazaret was located being chosen as the site; it was from the name of the monastery that the term ‘lazaretto’ developed. Initially designed for only 20 single rooms, the hospital was able to expand to 80 rooms when it was given a legacy in 1429; in order to cover the increasing financial costs, notaries had to expressly ask each testator from 1431 onwards whether he wished to leave something to the ‘locus Sanctæ Mariæ de Nazareth’ built ‘pro inspiratione diuina’. There were already discussions in 1456, when an epidemic was again raging in the city, about whether to establish a separate quarantine station in the lazaretto for those who had recovered from the plague, but whose return to everyday life was thought still to pose a risk to the city; but it was not until 1468, during another epidemic, that the ‘New Lazaretto’ was built on its own island for this purpose. Later, the old lazaretto was also increasingly used as a ‘quarantine station’, above all for arrivals from the Levant as well as for the purpose of quarantining and ‘disinfecting’ goods from overseas (see the contribution by Pia Doering in this dossier).
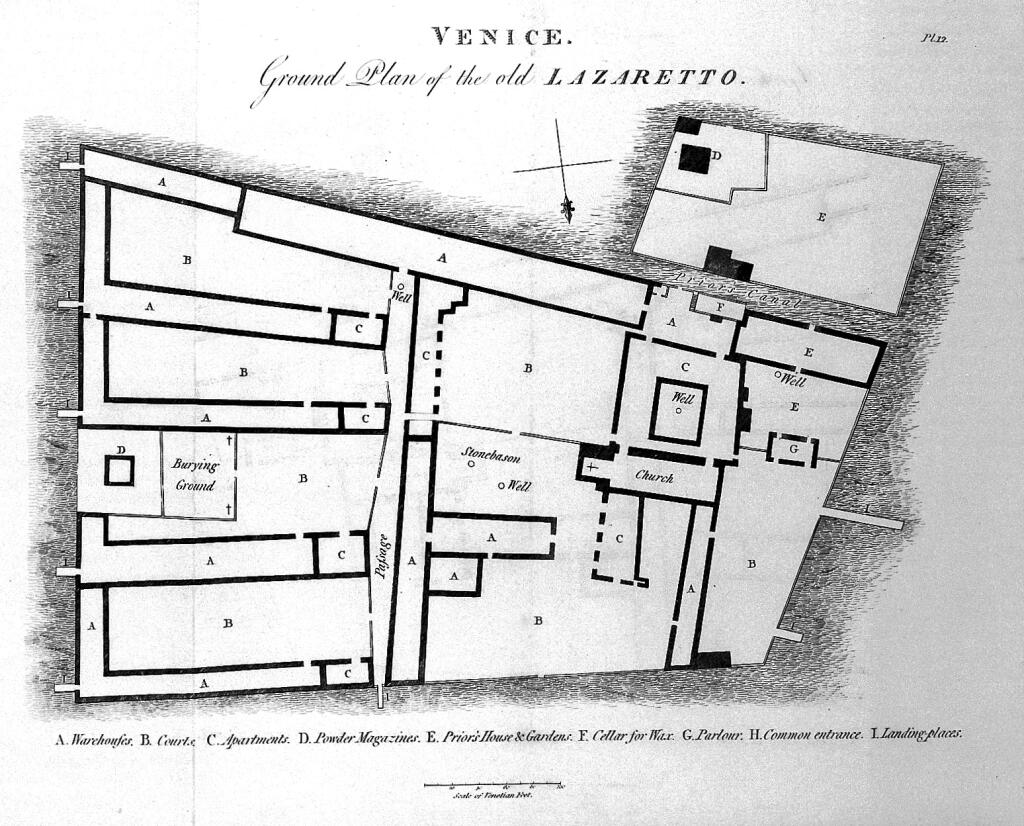
Although the lazaretto suffered considerable damage during its use as a military site from 1852 to 1967, we can gain a fairly good picture of its structures through the surviving buildings and two floor plans from 1789 and 1813. The Account of the Principal Lazarettos in Europe, published by the English prison and hospital reformer John Howard (1726-90) as the result of a study trip that had taken him from 1785 onwards (admittedly, long after the last major plague epidemics in Europe) to the best-known lazarettos in France and Italy as well as in Smyrna and Constantinople, also provides information on the organization and reality of life in the late 18th century.

The lazaretto island has the shape of an irregular trapezoid (Fig. 1). To the west is the church with its former enclosure, which was originally reserved as a generalato or fondaco for the Venetian representatives in Constantinople as well as the provveditors general and rectors from the Levant. Provost and provostess lived in the adjoining priory to the south-west, opposite which was the actual hospital building for people suffering from the plague and those who were possibly infected, which lined the southern flank of the island; it was converted into a warehouse to quarantine goods (tezzon vecchio) after the great plague epidemic of 1630 (Fig. 2). To the north, two more quarantine areas, the Crozzola and the Contumacia al Morer, were built in the 16th century, while the entire eastern half of the island comprises four L-shaped warehouses, built around a prato (meadow) as sections with pillar-supported roofs open to the south; to the east of the island was a powder magazine and a small cemetery. What is evident is the effort made to separate buildings, to create and maintain distances, and to isolate groups of people and goods from each other. Open, landscaped areas remain between elongated sections of buildings; each of the more recent tezzoni in the east had its own jetty: Howard (1789, 13) points out that “all these apartments have their separate entries and stairs, and every range of them has an open court in front”. The warehouses are half-open to allow free circulation of air (“that the air is not confined”).
The rules of life that applied in the lazaretto were also essentially aimed at avoiding contacts between groups, people and goods, and maintaining order on the island (in contrast to the institution in Saramago’s Blindness; see Martina Wagner-Egelhaaf’s contribution). If a suspicious case arose, the gates to the island had to remain locked; boats were not allowed to approach; all activities that provided people from different quarantine areas with the chance to meet were ceased. During his regular inspections, the prior had to carry a stick with him at all times in order to keep the internees at a distance. Internees could order their food as they wished at a fixed price, and the prior had to ensure that they were adequately supplied. Suppliers were not allowed to enter the lazaretto and had to use two-metre-long poles to hand out the baskets; their money had to be ‘disinfected’ in wine vinegar or salt water. Letters written in the lazaretto were fumigated by the warden of each respective apartment, and passed on by means of a stick with a split end to the prior, who perfumed them again and only then sent them out. Hygiene in the ‘apartments’ was by all accounts awful, though, Howard (1789, 11) describing the walls of his room as being “saturated with infection”, and surmising that they had not been cleaned for half a century.
“From peculiar paternal concern”: exclusion and demarcation in Austrian plague ordinances, 1654 and 1679
Besides Venice, the “city in the water” with its flourishing Levant trade, Austria and the imperial capital Vienna were among the regions of Europe particularly affected by the plague. In 1654, Emperor Ferdinand III issued “from peculiar paternal concern” a “New Infection Ordinance” (Vienna 1654). Based on older plague ordinances, it was aimed especially at rural areas. The reader of 2021 will be more or less familiar with many of the measures, but also the exceptions, that it lists: travellers from affected areas who could not prove by presenting a “credible document” or by swearing by “bodily oath” that “they had been in healthy and unsuspicious places for the previous forty days” had to self-isolate outside the country’s borders for 40 days. Should the plague break out in the country itself, appropriate rules were applied above all to Vienna and its suburbs, “or other places, especially where We or Our Young Sovereignty are at the same time with the Court” (6), thereby placing at the centre of the protective measures the monarch and the heir to the throne, on whom the future of the Habsburg countries depended! This regulation was relaxed when the supply chains to Vienna were endangered (“so that the commerce and supply of goods to the local city of Vienna is not disturbed [i.e. blocked], nor does a shortage occur because of this” [7]), in which case the regulation should apply only to the houses concerned and not to the whole locality. In order to allow business travel to Vienna while ensuring the necessary protection, the authorities designated several places of quarantine in the Lower Austrian quarters, where travellers were to self-isolate for forty days. This, then, specified a regulated quarantine district that was intended to shield a large area of the residential city.
In addition, the “New Infection Ordinance” provided for something like lockdown measures, which primarily affected the gastronomic sector and public festivals: since “gatherings are not a little dangerous, the authorities should stop them as much as possible, especially in the wine cellars, hostelries and Leuthgeb houses”, and church festivals, church events and fairs were prohibited during the infection period. There seems to have been no illusions about what could really be enforced. Gatherings for “honest weddings, child banquets, and other such festivities” could not be completely banned, but they were to be reduced “to the minimum” and held only “in clean, spacious, airy places and rooms”. In the event of a sharp increase in the number of deaths (“when death has taken over”), a stricter lockdown should apply, when “each and every gathering is to be stopped entirely, and the schools and baths to be closed” (14).
The year of the plague of 1679 saw the publication in Vienna of the “Plague Ordinance, or a useful report and expert opinion for the whole community” on the causes of the plague and measures taken to prevent its spread. The ordinance was taken from the estate of the emperor’s personal physician and professor of medicine, Johann Wilhelm Mannagetta (1588-1666), and published in a revised and edited form by the professor of medicine and personal physician to the empress dowager, Paul Sorbait (1624-91). Among the measures for spatial segregation and exclusion, it mentions “trusted lockers” who lock doors “with a mail lock”, “so that the people in the plague-stained house do not go out, or shock and infect other people” (115). The state’s plague ordinance of 1654 had already stipulated that affected houses be marked with a cross and thus marked out symbolically. But it was also the task of the “locker” to make sure that those locked in were cared for. Their spatial and social isolation continued even in death, for the deceased were to be carried unaccompanied to the graveyard and buried there “in a special place” in particularly deep pits. The ordinance of 1679 specified that the plague dead were to be carried to burial “not through the foremost alleys and squares, much less through the whole city, but to the nearest city gate through the alleys that are least inhabited”, and buried in the nearest graveyard “without any to-do in the alleys” (113). The plague was at least able to abolish this privilege of estate. In addition, this and a number of other measures show that the boundaries marked by the city wall and the keep were used to separate, if possible, the city itself from everything deemed unhealthy.
“How the lazaretto or plague house should be constituted”
The plague ordinance of 1679 also contained detailed information on what a lazaretto should be like (119-122). It should be “a commonly owned and public house or building, to which only those whom God has afflicted with the pestilence are directed”, and should be built “outside the city in the field (but not on the country road), where there are no houses for several steps, and on a quiet spot, and not in a valley, but where possible by a flowing body of water”. The windows should be “turned away from the city (so that its inhabitants will not be affected by the poisoned evil air)”, and if possible should only face north and east; a garden should serve those occupants who are mobile. The complex is to be divided into at least “three completely separated parts”: the first to accommodate “those suffering from the plague” in “several different rooms, parlours, chambers, and privies”, separated according to gender and with special “rooms” for the wealthy who pay for themselves; the second to be reserved for the healthy or those on the road to recovery (“several parts of whom already discharged”); the third to house officials and suspected cases. If overcrowding threatens, temporary huts are to be erected. Staff include a “pious, devout priest” for the spiritual care of those interned, an “obligated, forsworn, but compassionate lazaretto guardian and overseer”, and a doctor to attend to the wounds, a person to do shopping, a door guard, and others. Infected persons should be brought “into the lazaretto or plague house in the covered wagon by the wagoner appointed for this purpose”; those who refuse should be taken at least one mile outside the city or transferred to the plague house “by force”.

The Vienna lazaretto had been built in 1540-42 and was located in what is now the 9th district of Vienna, on the site of today’s Arne Carlsson Park. Situated about 900 m in front of the Viennese bastion on the little river Als, it certainly corresponded to the external requirements formulated in the plague ordinance of 1679 (Fig. 3, No. 7). Its structural appearance is only known in outline, as the lazaretto was converted into a soldiers’ hospital in 1766 and demolished in 1857. After two extensions, the complex comprised two wings at right angles to each other with five men’s rooms of 16 to 23 beds each, and four women’s rooms of 14 and 17 beds each, as well as four ‘melioration rooms’ with a total of 73 beds; an old chapel dedicated to St. John was also part of the complex. In 1657, a quarantine courtyard (Fig. 3, No. 6) was established a little closer to the city, which was a kind of ‘abating station’ for convalescents and those who had had contact with infected persons before they were allowed to return to the city after forty days. It thus had the same function as the Lazzaretto Nuovo in Venice.
“Gentlemen, I forget that I am in Europe”: cholera in Hamburg, 1892
The measures described so far were largely ephemeral in nature: they were only applied in cases of suspicion or after the outbreak of an epidemic, and created temporary distances between infected and healthy people, but hardly any permanent structures. This only changed in the course of the dramatic population growth of the large European cities during the 19th century, which often resulted in catastrophic housing conditions for the poorer sections of the population. After the plague had largely disappeared following the last wave that hit various parts of Europe between 1709 and 1720, from about 1830 it was cholera that found an ideal breeding ground, especially in the structurally overburdened large cities. It posed a danger that the measures of the 17th century could no longer deal with.
A devastating cholera epidemic broke out in Hamburg in mid-August 1892, killing more than 8,500 people in just under three months. It soon became clear that the housing conditions in the city had played a key role not only in the high mortality rate itself, but also in its very uneven distribution: for it was above all where people lived in particularly cramped conditions that the epidemic had taken its heaviest toll, with those districts of the city where the poorest sections of the population lived in often unrenovated old buildings being particularly affected. Robert Koch, who inspected the conditions in Hamburg as the official representative of the Reich Chancellor, recoiled in horror at what he found: “Gentlemen, I forget that I am in Europe”.
As historians Clemens Wischermann and Richard J. Evans in particular have pointed out, legislative measures focused in the following years on two areas: redeveloping neighbourhoods classified as unhealthy, especially the inner city near the harbour, and improving housing conditions in the long term. Issues of spacing and creating more space played a central role in this. There were constant delays, mainly due to the stubborn resistance shown by land and property owners who wanted to accept as few restrictions as possible. This only changed with the dockworkers’ strike in 1896, which brought into focus once again the miserable living conditions of the lower classes. After several attempts, a Housing Care Act was finally passed in 1907, which defined precise limits on the occupancy of flats and regulated the provision of toilets in particular. Thus, minimum values regarding air space were set for a dwelling: a child was allocated a minimum air space of 7.5 m3, and an adult, 15 m3. If these values are converted to today’s minimum living space height of 2.4 m, then this produces a floor space of 3.125 m2 per child and 6.25 m2 per adult – property and land owners had already fought in 1898 against values of 2 and 4 m2, arguing that a family of four, for example, could have made do with a living space of 12 m2! From then on, a maximum of 12 people or two families were allowed to share one toilet – before 1892, multi-storey houses sometimes had to make do with a single toilet in the courtyard.
Redevelopment occurred mainly in the so-called Gängeviertel, extremely dense residential quarters near the harbour, many of which could only be accessed via those narrow alleys that had particularly shocked Koch (https://www.hamburg.de/geschichte/4643766/gaengeviertel-hamburg/#detailLayer). Demands arose as late as November 1892 for their demolition in favour of wide streets and healthy flats, and at the beginning there was also the intention to reallocate them to the previous residents. However, the dockworkers’ strike shifted perspectives: the “airless, lightless and loveless Gängeviertel”, according to the Hamburg Correspondent, were now reinterpreted as hotbeds of criminality and brutality, these attributes being applied to those living there; and, in line with a traditional metaphor, the risk to health associated with them was now paralleled with the risk to the socio-political order of the city. In the end, the rents in the newly built flats in the redeveloped quarters were so high that none of the families who had lived in the southern Neustadt, for example, were able to return to the neighbourhood. Most had to look for a new place to live in the modern apartment buildings that were now being built. While these buildings offered more light and more space and thus healthier living conditions, this came at a price: long distances to work (to which the construction of the elevated railway was a response), as well as the loss of home and familiar surroundings. This also affected the villa districts of the upper middle classes, who in turn moved to more remote suburbs. The cholera epidemic and its consequences – these shaped the spatial planning of the city far beyond the protective measures originally intended.