|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Free Neuropathology 6:6 (2025) |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Original Paper |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Capillary basal lamina in human brain and spinal cord has fibrillar collagen type I and type III: Ignorance may not be bliss |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Wen-Lang Lin1, Dennis W. Dickson1 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
1 Department of Neuroscience, Mayo Clinic, Jacksonville, Florida, USA |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Corresponding author: |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Additional resources and electronic supplementary material: supplementary material |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Submitted: 18 December 2024 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Keywords: Capillary basal lamina, Fibrillar collagens, Central nervous system, Electron microscopy, Immunohistochemistry, Species difference |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Abstract The capillary basal lamina (BL) located between the endothelial cell, pericyte and perivascular astrocyte plays important roles in normal and diseased central nervous system (CNS). Using immunohistochemistry (IHC), electron microscopy (EM) and post-embedding immunogold EM (IEM), we studied capillary BL in biopsy and autopsy tissues of human CNS from cases with and without significant brain pathology and aged from 4 days to 49 years. In all cases, IHC showed, in the BL of microvessels, immunoreactivity for collagen types I, III, IV, VI and fibronectin. EM revealed fusion of the BL of capillary endothelial cells or pericyte with perivascular astrocyte BL, which was focally split, resulting in expanded spaces bordered by BL and containing striated fibrils. There was no significant thickening of fused or split BL. IEM showed localization of collagen I and III to banded fibrils, and of collagen IV to split and fused BL. These characteristic ultrastructural findings in human capillary BL were not found in normal or transgenic mice. Our observations of fibrillar collagen in young individuals complement previous observations of similar findings in older individuals. This raises the possibility that fibrillar collagen in human vascular BL plays a significant role in CNS capillary physiology and pathophysiology. The species-specific differences in capillary morphology between humans and mice might have relevance to poor correlations between benefits of immunotherapy and drug treatment in mice compared with human. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
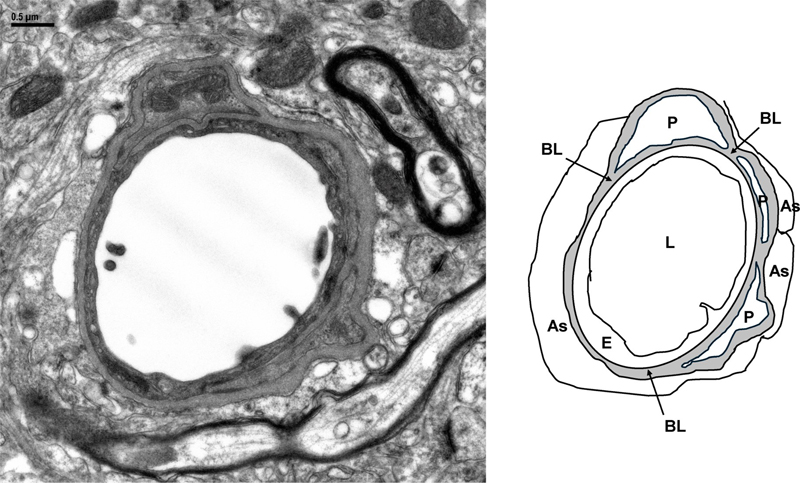
Introduction Capillaries are the smallest segment of the vascular network throughout the body and play crucial roles in exchange of oxygen, nutrients, pharmaceuticals, and waste between vascular and perivascular tissues [1]. Electron microscopic (EM) studies show capillary lumens are covered by a single layer of endothelial cells and the abluminal side is covered by a basal lamina (BL, basement membrane], which is formed by the fused BL of endothelial cells and pericapillary astrocytes [2–4]. Pericytes and their processes are present focally in the fused BL. Fig 1 illustrates the anatomical relationship between capillary lumen, endothelial cell, pericyte, pericapillary astrocyte, and basal lamina.
Fig 1. Electron micrograph of a capillary in cross section from the cortex of a 5.5-month-old non-Tg mouse. Perfusion of fixative cleared the lumen (L) that is lined with a thin layer of endothelial cells (E) abutting a homogenous basal lamina (BL), Pericapillary astrocytes (As) and their end-feet are tightly attached on the other side of the BL. Pericyte (P) and its processes are embedded in the BL. The sketch illustrates the anatomical relationship between vascular cells and BL. In the central nervous system (CNS), capillary endothelial cells have specific structures that control movements of molecules between the blood and brain parenchyma to maintain homeostasis of the CNS [5], as well as regulation of blood flow [6]. These structures include interendothelial tight junctions, luminal and abluminal molecular transporters, and a paucity of vesicular transport, which constitutes the blood-brain-barrier (BBB). Pericytes are also involved in BBB function and blood flow [7, 8]. EM of well-preserved/fixed mouse and rat CNS has made this ultrastructural definition of the capillary BBB universally accepted in other animal species. The non-cellular capillary structure, BL, sandwiched between the abluminal side of endothelial cells and pericapillary glial cells, also plays a key role in barrier functions and immune response in the CNS [9–11]. Early biochemical studies of BL from non-CNS tissues of human and mouse have identified major and minor components and their molecular interactions [12]. Non-fibrillar collagen type IV [Col 4] is biochemically the most abundant component of BL. Col 4 interconnects with non-collagenous components, including laminin, perlecan, nidogen and fibronectin, to form an amorphous meshwork with a homogeneous density on EM. These biochemical data, like morphological data, are also accepted universally. The Col 4-dominant biochemical view also prevails in CNS capillary BL. Compared to Col 4, other BL components are understudied [13]. Early studies in rats have shown that BL could be a physical barrier to certain intravenously injected molecules after they pass the BBB [14, 15]. It is hypothesized that electric charges of BL components contribute to barrier function. Investigators have tried to translate data from mouse models of human disease to clinical trials in humans; however, such translational studies have often not succeeded. The difference between human and mouse capillaries may contribute to this finding. Intravenously administered molecules that can bypass BBB have some success treating mouse models of human neurodegenerative diseases but have minimal effect in humans for currently unknown reasons, and the role of vascular cells and BL needs to be considered. Recent studies have shown differences in brain cells and microvascular cells between humans and mice. Significant differences in expression were found in specific brain regions [16–20]. Similar studies have not been performed in human and mouse spinal cords. The differences in expression in cell types between species could produce different BL properties in human and mouse CNS, which might interfere with the movement of molecules/drugs within the perivascular compartment. Fifty years ago, Cervós-Navarro and Ferszt [21, 22] described ultrastructural characteristics of capillaries in human spinal cords of individuals ranging in age from 7-months to 97 years. They found a consistent “dilated pericapillary space” bordered on one side by endothelial BL and on the other side by perivascular glial cells, with collagen fibers in about 70 % of the capillaries. In 1998, Ono et al. [23] studied spinal cord capillaries in patients ranging in age from 37 to 74 years with sporadic amyotrophic lateral sclerosis (sALS), other neurologic diseases and in neurologically normal controls. They found that about 40 % of capillaries in the three groups had a “focally split BL to encompass a large area containing accumulation of collagen fibrils.” In 2012, Garbuzova-Davis et al. [24] described expanded capillary BL with collagen fibrils in spinal cords of 18 controls [39–86 years] and in sporadic ALS [45–83 years]. In 2013, we showed similar findings in a preliminary report of 8 controls (28–81 years), 5 sALS (47–75 years) and 7 familial ALS (15–69 years) patients [25]. In 2015, Sasaki [26] examined 358 and 366 capillaries in 12 controls (50–80 years) and 12 sALS (59–83 years) cases and found “slight or abundant accumulation of collagen fibers in the perivascular space within expansion of the capillary basement membrane” in controls and ALS cases. Expanded spaces in BL of spinal cord capillaries have not been reported in normal mice or ALS mouse models. In contrast to spinal cord capillaries, early EM studies of human cerebral capillaries only briefly comment on collagen fibrils in BL, with a few images: 61-year-old [27], age unknown [28], fetus [29, 30], 50–66 years [31], 56 years [32] and age unknown [33]. Splitting of the BL has also been observed in capillaries of biopsy tissues from patients with cerebral edema (58–80 years) [34], multiple sclerosis (25–30 years) and Alzheimer’s disease (AD) (age unknown) [35, 36]. Later, Farkas et al [37] examined human cerebral periventricular white matter and showed collagen fibrils within capillary BL in patients 40 to 90 years of age. They also reported increased BL pathology in AD and Parkinson’s disease. Szpak et al [38] showed cerebral capillaries with numerous collagen fibers in two AD patients (36–46 years) with a p.P117L PSEN1 mutation. They all showed banded collagen fibrils with EM. In a preliminary EM report of human brain capillary BL (11 cases, 7–49 years of age), we showed banded collagen in expanded spaces in the basal lamina [39]. Some studies have reported collagen types other than Col 4 in human brain capillaries. van Duinen et al [40] showed immunohistochemical (IHC) staining of collagen type I (Col 1) and collagen type III (Col 3) and fibronectin in capillaries of normal controls aged 36–78 years. Dong et al [41] studied six patients (46–83 years old) with cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy with NOTCH 3 mutations (CADASIL) and six controls (54–82 years old). They found Col 1 and Col 3 in capillaries of both CADASIL and control cases. Staining was heterogeneous with much lower frequency and intensity in controls. In our preliminary EM reports of human CNS capillary BL, IEM localized Col 1 and Col 3 to fibrillar collagens in the expanded spaces [25, 39]. IHC and proteomic analysis showed Col 6α3 in controls, AD and cerebral amyloid angiopathy (CAA) and Col 6ɑ2 in individuals with CAA ranging in age from 65–95 years [42], and Col 1ɑ1 in AD with CAA ranging in age from 58–97 years [43], and in all vessels of CAA cases ranging from 61–83 years old [44]. The sparse EM studies of CNS capillary BL in young human cases prompted our studied of capillary BL with IHC, EM and IEM in cases ranging in age from 4 days to 49 years. The cases had no significant brain pathology or a range of neurological disorders. We limited the study to those 50 years of age or younger to minimize the possible effects of age-related neurodegenerative or cerebrovascular changes [45, 46]. Additionally, considering the increased attention on species differences between brain vasculature of humans and mice [19, 20, 47], we included normal and transgenic (Tg) mouse models of human neurodegenerative diseases. Material and Methods Brains and spinal cords Table 1 listed human brains and spinal cords from the brain bank in Mayo Clinic, Jacksonville, FL. A total of 45 cases aged from 4 days to 49 years old that included 18 cases with no significant brain pathology and 27 cases with different neurological disorders. Among them were two biopsies and 10 cases with postmortem interval (PMI) of less than 24 hours. Neuropathologic assessments were based on light microscopic examination of paraffin sections. Table 2 CNS tissues were from non-Tg and Tg mice developed in Mayo Clinic, Jacksonville, FL [48–50].
Antibodies Affinity purified rabbit antibodies to Col 1, Col 3, Col 4 (Rockland, Limerick, PA; Chemicon, Temecula, CA), Col 6A1 (Atlas Antibodies, American Research Products, Inc., Waltham, MA), and to plasma fibronectin (F3648, Sigma, St. Louis, MO), Monoclonal mouse antibody to Col 4 (MP Biomedicals, Solon, OH; Chemicon, Temecula, CA). Goat anti-rabbit IgG conjugated with 10- or 18-nm colloid gold particles (Jackson ImmunoResearch Laboratories, West Grove, PA). Immunohistochemistry Formalin-fixed human and mouse tissues were processed for paraffin embedding by a TissueTek Embedding Console System, TEC5 (Sakura Finetek USA, Inc., Torrance, CA). Five μm-thick sections mounted on Fisherbrand Plus glass slides were pre-treated in a steamer with deionized water before immunostaining with an autostainer (DAKO, Carpinteria, CA) using 3,3’-diaminobenzidine as the chromogen. Sections are examined with an Olympus BX 50 fitted with an Olympus DP12 digital camera. Electron Microscopy Small pieces (2 x 2 m2) of formalin-fixed human tissues were further fixed in 2.5 % glutaraldehyde-2 % paraformaldehyde in 0.1 M cacodylate buffer. Biopsy tissues were directed fixed in the above fixative. Mice were perfused transcardially with saline followed by 2.5 % glutaraldehyde-2 % paraformaldehyde in 0.1 M cacodylate buffer. All tissues were fixed overnight at 4 °C. The tissues were processed for embedding in Epon as previously described [48, 51]. Ultrathin sections were collected on Formvar-coated copper grids, stained with uranyl acetate and lead citrate, and examined with a Philips 208S electron microscope (FEI, Hillsboro, OR) fitted with a Gatan 831 Orius camera (Gatan, CA), and a JEM-1400 Flash microscope (JEOL, Peabody, MA). Digital images were processed with Adobe Photoshop software. Post-embedding Immunogold EM Formalin-fixed tissue pieces (2 x 2 mm2) were processed for embedding in LR White resin, and subjected to IEM as previously described [48, 51]. For fibronectin, ultrathin sections collected on Formvar-coated nickel grids were pre-treated by floating with section-side down on 1 ml of 0.1 M sodium citrate, pH 6, for 10 min at 95 °C and cooled to room temperature for 15 minutes before incubation with antibody. Results Only selected figures were described here; more figures can be found in Supplementary Material. The morphological descriptions were similar, if not the same, in all cases, regardless of age, sex, disease, tissue region and PMI. In this report capillary refers to vessels less than 10 μm in diameter. Fig 1 shows an EM of a capillary from the cortex of a normal 5.5-month-old mouse illustrating the anatomical relationship between the vascular cells and BL. IHC of the same large vessels (arterioles) in serial sections established the specificity of antibodies. Sections of cerebral cortex, cerebellar vermis, and spinal cord anterior horn in Figs 2–4 show Col 4 outlined endothelial BL and the outermost vascular BL, but not the media or adventitia, which were immunostained with Col 1 and Col 3. Vascular media in large vessels normally contains smooth muscle cells surrounded by fibrillar Col 1 and Col 3. Adventitia is the outermost area of large vessels that also contains fibrillar collagens.
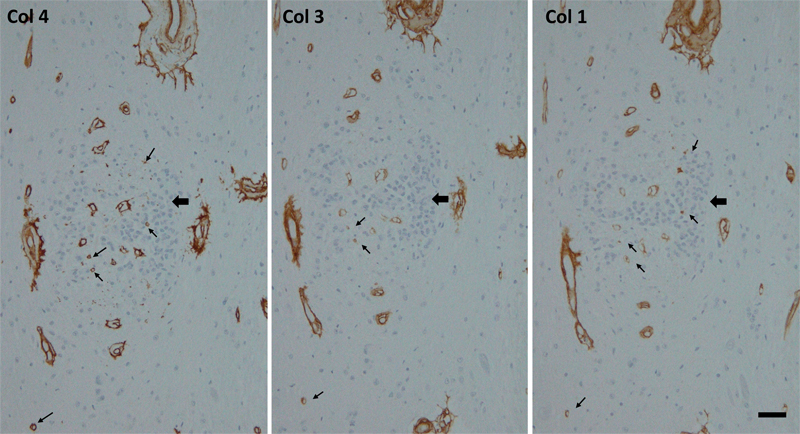
Fig 2. 18-year-old male with no significant brain pathology. Mid-frontal cortex. Postmortem interval, 18 hours. Immunohistochemistry of collagen type I, III, and IV (Col 1, Col 3, Col 4) in serial sections of the same field (cortex next to a deep sulcus, arrowheads) showing many microvessels stained with Col 4. However, several microvessels (arrows) are also stained with Col 1 and Col 3 with stronger Col 3 than Col 1 staining. Staining of Col 3 and Col 1 but not Col 4 to the adventitia of small arterioles (curved arrows) and leptomeningeal vessels (arrowhead) indicate specificity of antibodies. Vascular adventitia and leptomeningeal vessels normally contain fibrillar collagens, e.g., Col 1 and Col 3. Scale bar, 50 μm.
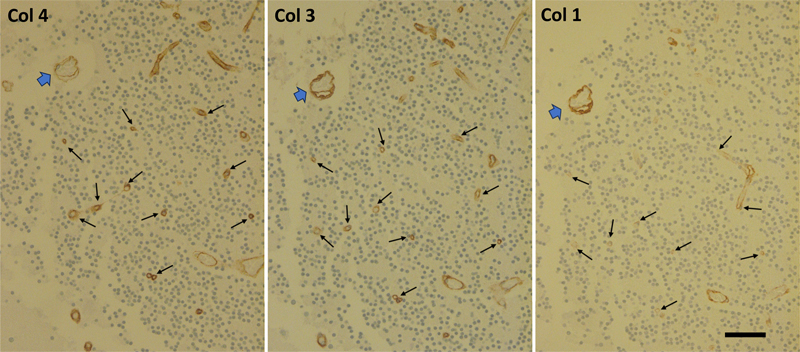
Fig 3. 16-year-old male with no significant brain pathology. Cerebellum, vermis, granular layer. Immunohistochemistry of collagen type I, III, and IV (Col 1, Col 3, Col 4) in serial sections of the same field with arrowheads pointing to the same large vessel. Many Col 4-stained microvessels are also stained with Col 3 and Col 1, with Col 3 being stronger (arrows). Note in the large vessel, Col 4 outlines the vessel and the endothelial basal lamina, while Col 1 and Col 3 stained the media that normally contains fibrillar collagens surrounding vascular smooth muscle cells. Scale bar, 50 μm.
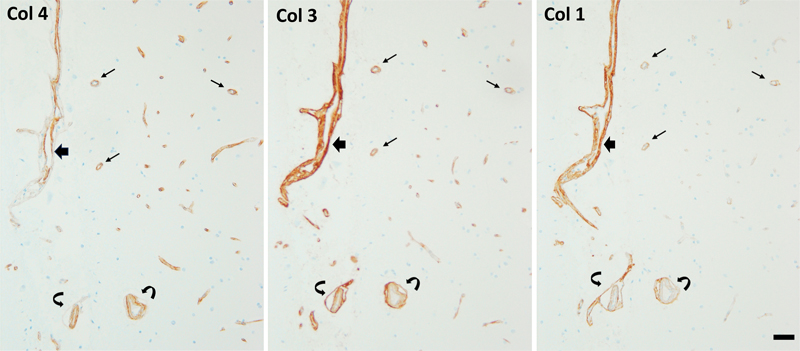
Fig 4. 38-year-old male with amyotrophic lateral sclerosis. Spinal cord. Immunohistochemistry of collagen type I, III, and IV (Col 1, Col 3, Col 4) in serial sections of the same field near central canal epithelium (arrowheads). Note some of Col 4-stained microvessels are also stained with Col 3 and Col 1 (arrows). In the large vessels, Col 4 outlines the vessel and the endothelial basal lamina, while Col 1 and Col 3 stained the media that normally contains fibrillar collagens surrounding vascular smooth muscle cells. Scale bar, 50 μm. As would be expected, IHC of Col 4 showed immunostaining of many microvessels in various cerebral regions, cerebellar vermis and spinal cord as Col 4 is the major BL component. Importantly, in all cases, many of the same vessels in serial sections were also immunostained strongly for Col 3 and weakly for Col 1. EM (Figs 5–13) and IEM (Figs 14–22) confirmed the IHC findings of microvessels. Cross sections of capillaries were selected to ensure their proper orientation for measurement of diameter and their ultrastructural organization. Like capillaries in non-CNS regions of the human body, CNS capillaries have luminal endothelium and abluminal BL with pericytes embedded within the BL. The BL were composed of a homogeneous structure representing the fused BL of endothelial cell/pericyte and perivascular astrocyte. Also observed were segments with apparent splitting of the BL (Fig 5). Some of the split BL were shown to be continuous with fused BL in the same section. The most striking finding was the small to large amounts of fibrils deposited in various focally expanded spaces bounded by split BL. These fibrils displayed characteristic banding patterns of fibrillar collagens, with a width ranging from 50–80 nm diameter. Sometimes, collagens larger than 120 nm were found (Fig 8, Supplementary Fig 32). All fibrils appeared randomly oriented in the expanded space. Very sparse cytoplasmic elements were present in the expanded space. Tissues from short PMI autopsies and biopsies showed pericapillary parenchyma tightly wrapping the capillaries, even in areas with massive, banded collagen deposits (Fig 10, Supplementary Figs 26, 41, 57). No banded fibrils were observed outside of the BL. No phagocytotic cells or inflammatory cells were present. There was minimal astrogliosis, and despite autolytic changes, astroglial processes maintained hemi-desmosome attachments on fused or split BL (Fig 20–22, Supplementary Figs 55) [52]. There was no evidence of extensive BL remodeling (e.g., duplication or thickening) of either fused or split BL.
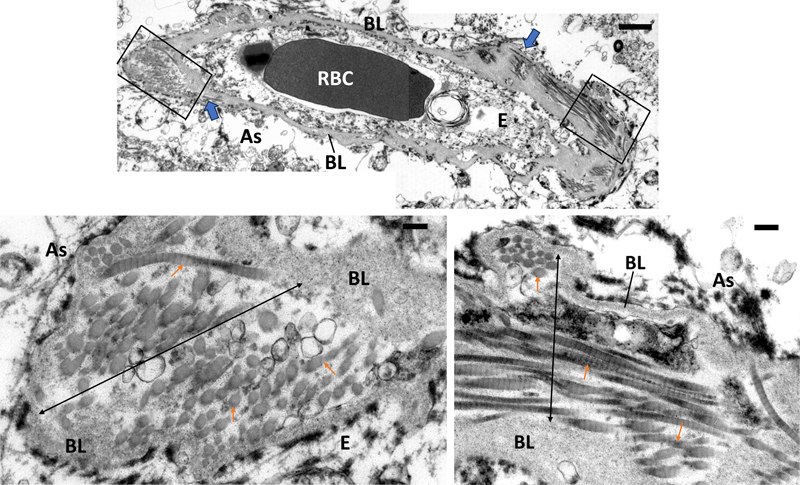
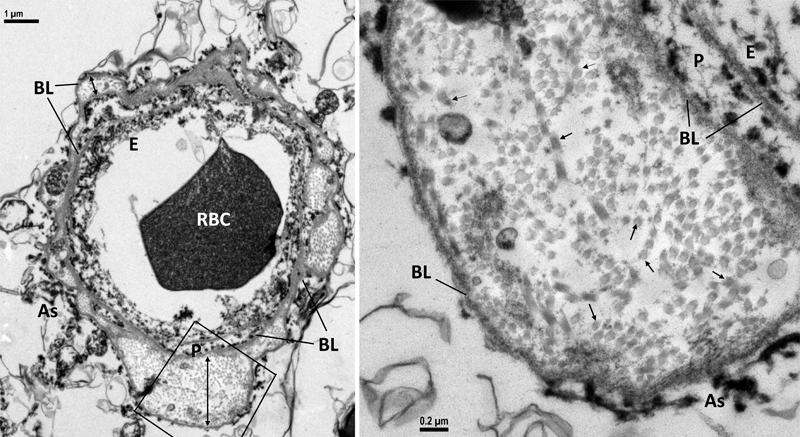
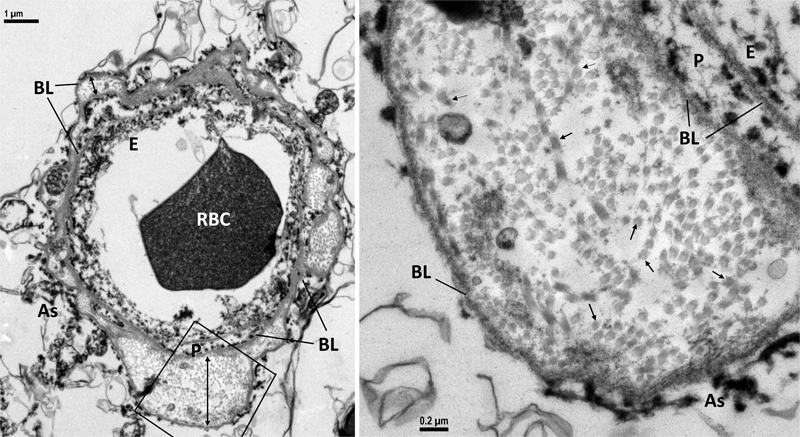
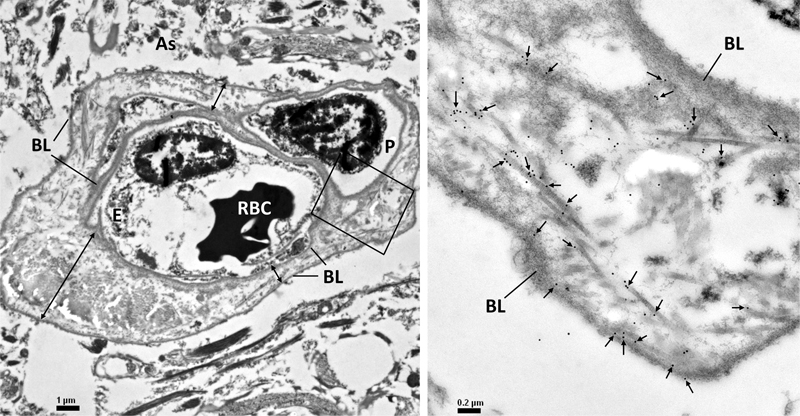
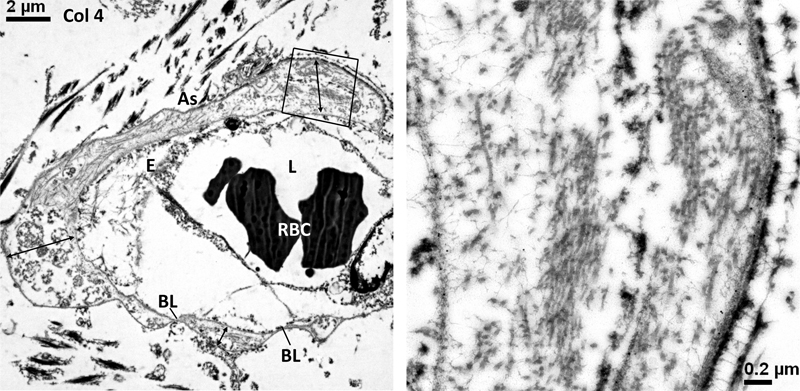
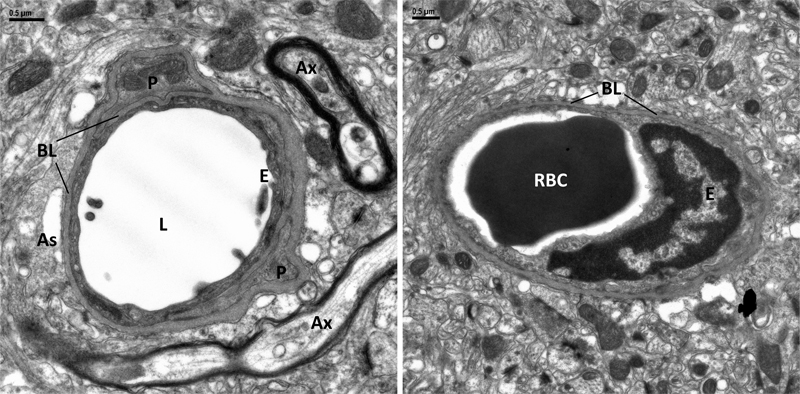
Fig 5. 9-year-old male with tauopathy, neurofilament inclusion disease, motor neuron disease. Cingulate. Top. Electron micrograph of a capillary at low magnification showing fused basal lamina (BL) of endothelial cell (E) and perivascular astrocyte (As) at the top and bottom, and split BL at the left and right side of the capillary. Arrowheads point to split of fused BL. RBC, red blood cell in capillary lumen. Bottom. Enlargements of boxed areas showing expanded spaces [double head arrows] in the split BL contain bundles of banded fibrils in cross, oblique and longitudinal sections [arrows]. Scale bars, top, 1μm; bottom, 0.2μm.
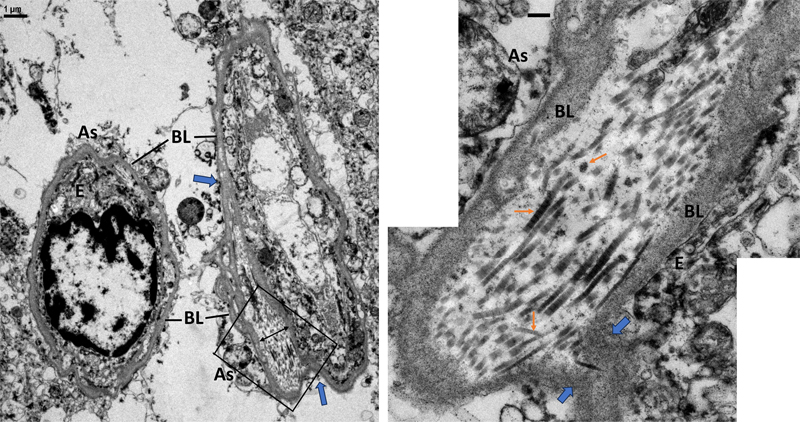
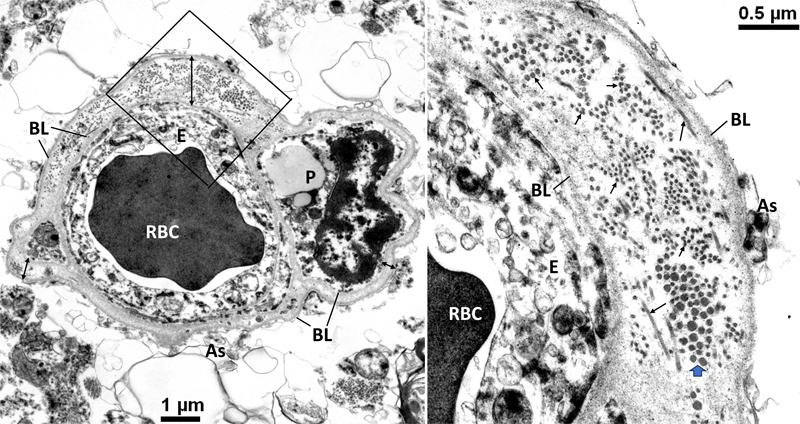
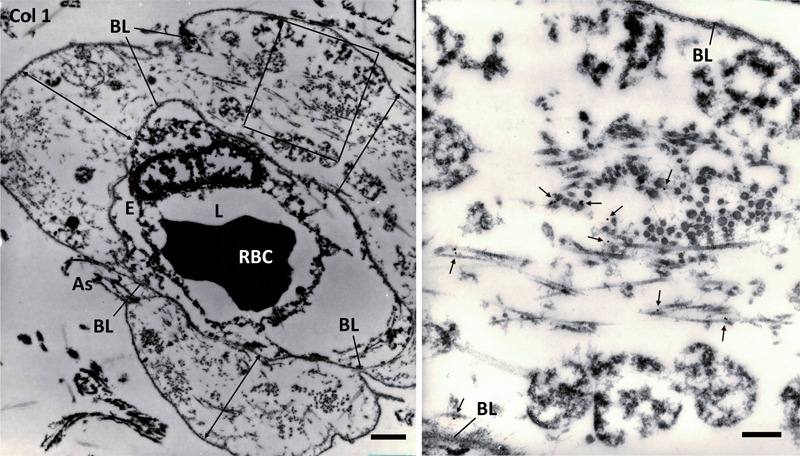
Fig 6. 18-year-old male with no significant brain pathology. Superior frontal cortex. Postmortem interval, 18 hours. Same case with IHC depicted in figure 2. Left. Electron micrograph of two capillaries with homogenous fused basal lamina (BL) of endothelial cell (E) and perivascular astrocyte (As). Note the right capillary has an expanded space [double head arrow] formed by split BL (arrowheads). Right. Enlargement of boxed area shows the expanded space containing many banded fibrils (arrows) in random orientation. Arrowheads indicate splits of the two BLs. Scale bar, right, 0.2μm.
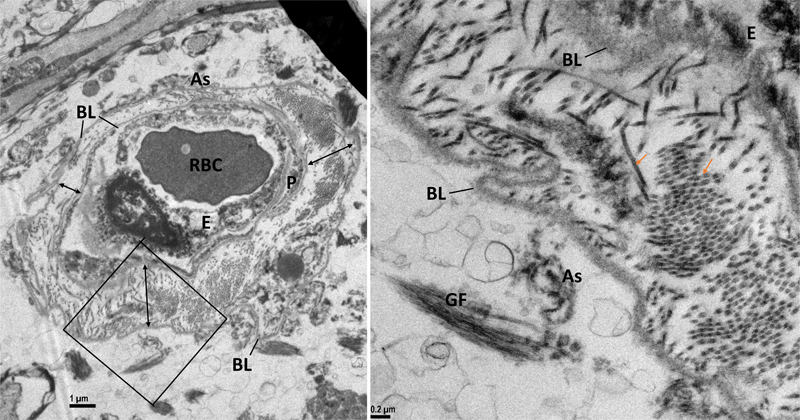
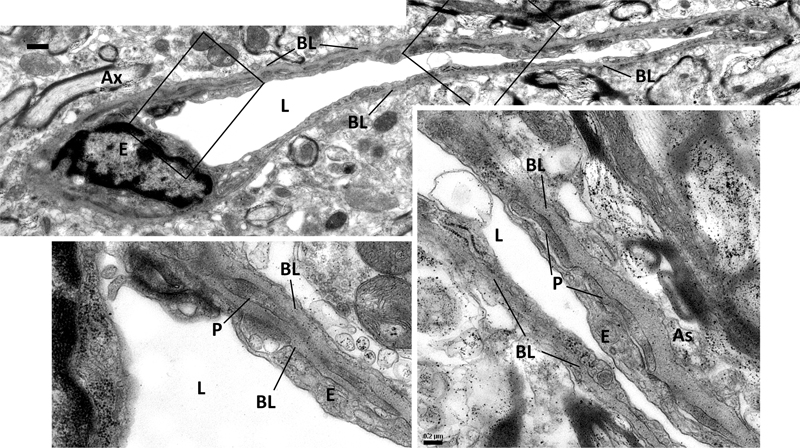
Fig 7. 28-year-old male with congenital dopamine β-hydroxylase deficiency, but no significant brain pathology. Spinal cord. Left. Cross section of a capillary completely wrapped by expanded spaces [double head arrows] in split basal lamina (BL) of the endothelial cell (E), pericyte (P) and perivascular astrocyte (As). Right. Boxed area is enlarged to show the expanded space filled with cross and longitudinal sections of banded fibrils (arrows). RBC, red blood cell occupying the capillary lumen. GF, astrocytic glial fibrils.
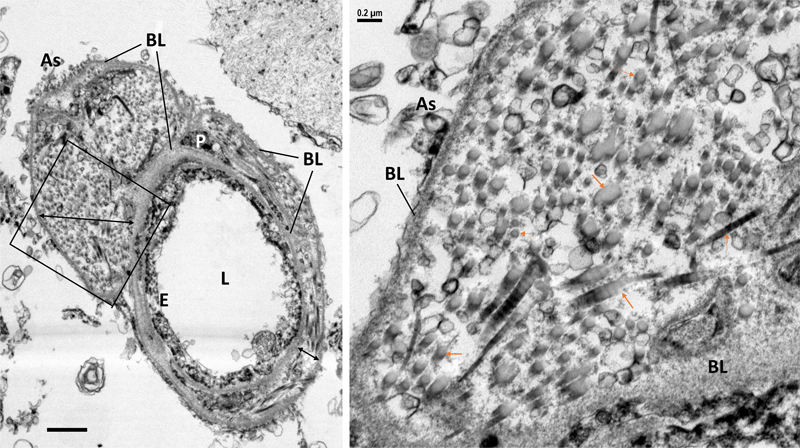
Fig 8. 33-year-old male with acute contusion of frontal and temporal lobes, but no other significant brain pathology. Substantia nigra. Postmortem interval, 21 hours. Left. A capillary with split basal lamina (BL) of endothelial cell (E), pericyte (P) and perivascular astrocyte (As) forming wide and narrow expanded spaces (double head arrows) filled with fibrils. L, capillary lumen. Scale bar, 1μm. Right. Enlarged boxed area showing large and small banded fibrils in cross and longitudinal sections (arrow) in the expanded space.
Fig 9. 41-year-old female with no significant brain pathology. Superior frontal cortex. Left. Cross section of a capillary with large and small expanded spaces (double head arrows) between split basal lamina (BL) of endothelial cell (E), pericyte (P) and perivascular astrocyte (As). RBC, red blood cell in the capillary lumen. Right. Enlarged box area shows many banded fibrils [arrows] in the expanded space.
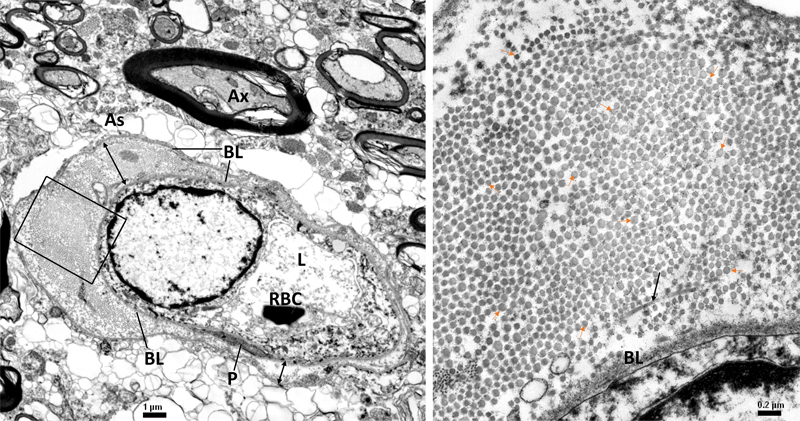
Fig 10. 41-year-old female with amyotrophic lateral sclerosis with chromosome 9 open reading frame 72 (C9ORF72) mutation. Spinal cord. Postmortem interval, 3 hours. Left. Cross section of a capillary with large and small expanded spaces (double head arrows) between split basal lamina (BL) of endothelial cell (E), pericyte (P) and perivascular astrocyte (As). RBC, red blood cell in the capillary lumen (L). Ax, myelinated axon. Right. Enlarged box area shows the large, expanded space is filled with many fibrils in cross-sections (arrows), and a longitudinal banded fibril (long arrow).
Fig 11. 44-year-old male with Perry’s syndrome. Substantia nigra. Postmortem interval, 7 hours. Left. Cross section of a capillary enwrapped with large and small expanded spaces (double head arrows) due to separation of basal lamina (BL) of the endothelial cell (E), pericyte (P) and perivascular astrocyte (As). RBC, red blood cell in capillary lumen. Right. Enlarged boxed area shows the expanded space contains longitudinal banded fibrils [long arrows] among many cross-sectioned fibrils (short arrows). Note some large-diameter fibrils in cross sections (double arrows). The split BL are not thickened.
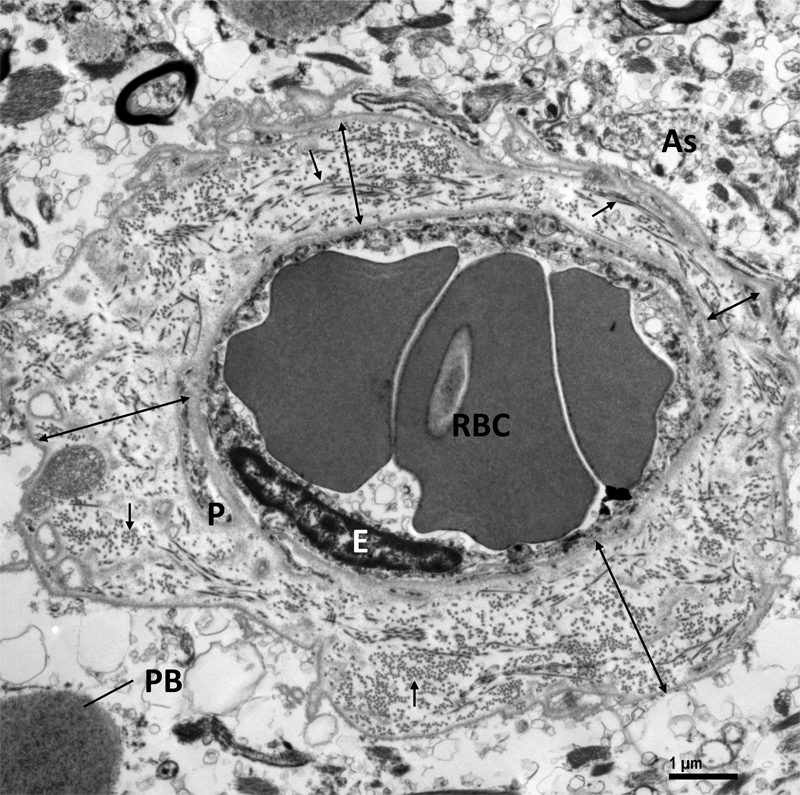
Fig 12. 48-year-old female with polyglucosan body disease. Optic tract. Cross section of a capillary with large and small expanded spaces (double head arrows) between split basal lamina (BL) of endothelial cell (E), pericyte (P) and perivascular astrocyte (As). The expanded space is filled with fibrils in cross- and longitudinal sections (arrows). RBC, red blood cell in the capillary lumen. PB, polyglucosan body.
Fig 13. 49-year-old male with diffuse Lewy body disease (DJ-1 mutation). Basal nucleus of Meynert. Left. Cross section of a capillary with fused and split basal lamina (BL) of endothelial cell (E), pericyte (P) and perivascular astrocyte (As). RBC, red blood cell in the capillary lumen. Right. Enlarged box area shows the expanded space between split BL (double head arrow) contains a few longitudinal banded fibrils (long arrows), many cross-sectioned fibrils in various diameters [short arrows] and a cluster of small fibrils.
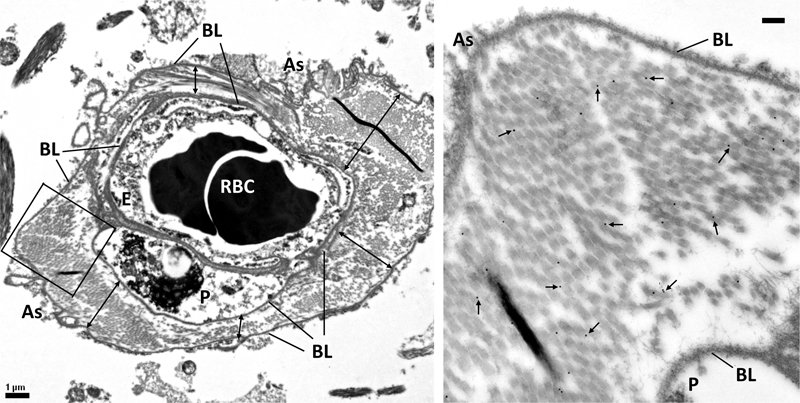
Fig 14. 28-year-old male with congenital dopamine β-hydroxylase deficiency but no significant brain pathology. Spinal cord. Immunogold electron micrographs of collagen type I (Col 1). Left. Cross section of a capillary enclosed completely by wide (left and right side) and narrow (top and bottom) expanded spaces between the basal lamina (BL) of endothelial cell (E), pericyte (P) and perivascular astrocyte (As) (double head arrows). The space is filled with fibrils. RBC, red blood cells in the capillary lumen. Right. Enlargement of boxed area showing localization of Col 1 to the fibrils. Arrows point to gold particles. Note the absence of gold particles from the split homogeneous BL of As and P. Scale bar, right, 0.2μm.
Fig 15. 28-year-old male with congenital dopamine β-hydroxylase deficiency and no significant brain pathology. Spinal cord. Immunogold electron micrographs of collagen type III (Col 3). Left. Cross section of a capillary with a very wide expanded space [double head arrows] between the split basal lamina (BL) of endothelial cell (E), pericyte (P) and perivascular astrocyte (As). The space is filled with fibrils. The lower half of the capillary has narrow spaces between the split BL. RBC, red blood cell in the capillary lumen. Right. Enlargement of boxed area showing localization of Col 3 to the fibrils. Arrows point to gold particles. Note the absence of gold particles from the split homogeneous BL of As and E. Scale bar, left, 1μm.
Fig 16. 28-year-old male with congenital dopamine β-hydroxylase deficiency, no significant brain pathology. Spinal cord. Immunogold electron micrographs of collagen type IV (Col 4). Left. Cross section of a capillary with wide and narrow expanded spaces (double head arrows) between the split basal lamina (BL) of endothelial cell (E) and perivascular astrocyte (As). The spaces are filled with fibrils. RBC, red blood cell in the capillary lumen. Right. Enlargement of boxed area showing localization of Col 4 to the homogeneous split BL of E and As, but not the banded fibrils in the expanded space. Arrows point to gold particles.
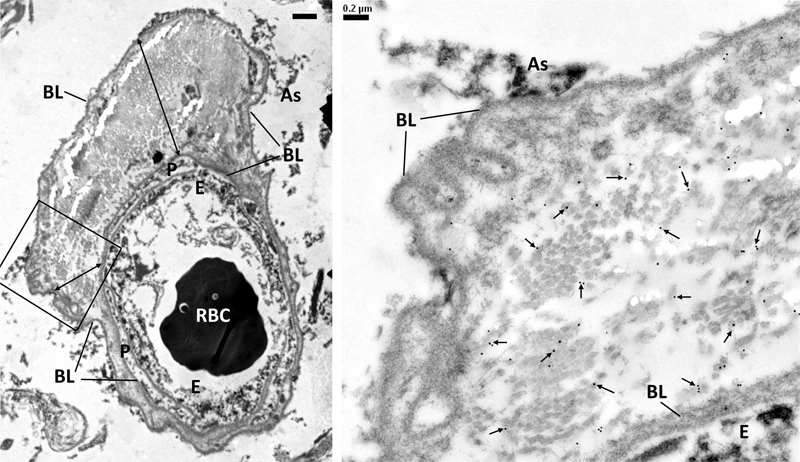
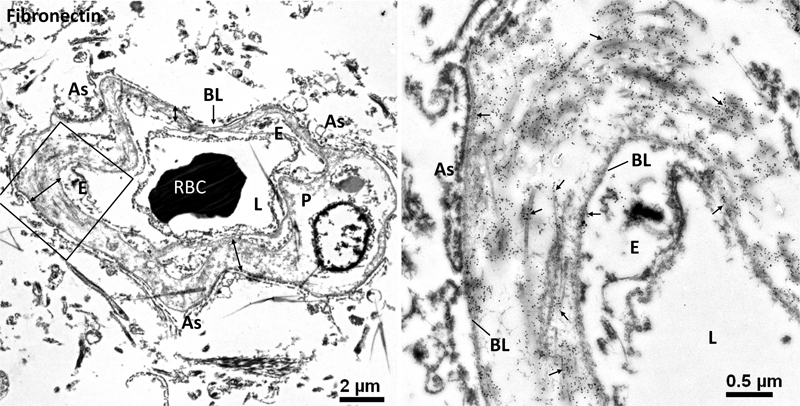
Fig 17. 28-year-old male with congenital dopamine β-hydroxylase deficiency and no significant brain pathology. Spinal cord. Immunogold electron micrographs of fibronectin. Left. Cross section of a capillary with wide and narrow expanded spaces [double head arrows] between the split basal lamina (BL) of endothelial cell (E), pericyte (P) and perivascular astrocyte (As). The spaces are filled with fibrils. RBC, red blood cell in the capillary lumen. Right. Enlargement of boxed area showing localization of fibronectin mostly to the fibrils in the space, but also to the homogeneous split BL. Arrows point to gold particles.
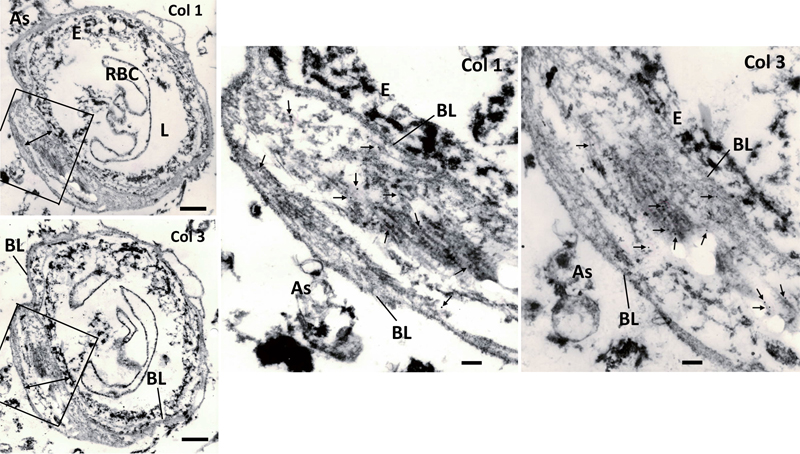
Fig 18. 42-year-old male with familial Parkinson’s disease. Putamen. Immunoelectron micrographs of collagen type I (Col 1) and type III (Col 3). Left. Serial sections of a capillary with fused and split basal lamina (BL) of endothelial cell (E) and perivascular astrocyte [As]. Double head arrows indicate expanded spaces between the split BL. RBC, ghost red blood cell in capillary lumen (L). Middle, right. Enlargements of respective boxed area. Gold particles (arrows) are localized mainly to banded collagen fibrils in the expanded space and rarely to the split thin BL surrounding the space. Scale bar, left, 1 μm; middle, right, 300 nm.
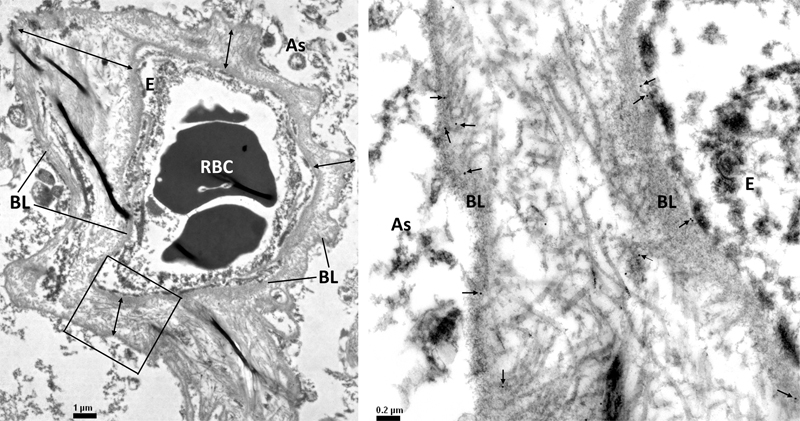
Fig 19. 46-year-old female with hereditary diffuse leukoencephalopathy with spheroids. Frontal cortex white matter. Immunogold electron micrographs of collagen type I (Col 1). Left. Cross section of a capillary showing fused basal laminas (BL) of endothelial cell (E) and perivascular astrocyte (As) splits and the resulting expanded spaces [double head arrows] with fibrillar deposits. RBC, red blood cell in capillary lumen (L). Right. Enlargement of boxed area reveals localization of Col 1 (arrows pointing to gold particles) to longitudinal banded fibrils and cross-sectioned fibrils in the expanded space, but not the split thin BL. Scale bars, left, 1 μm; right, 300 nm.
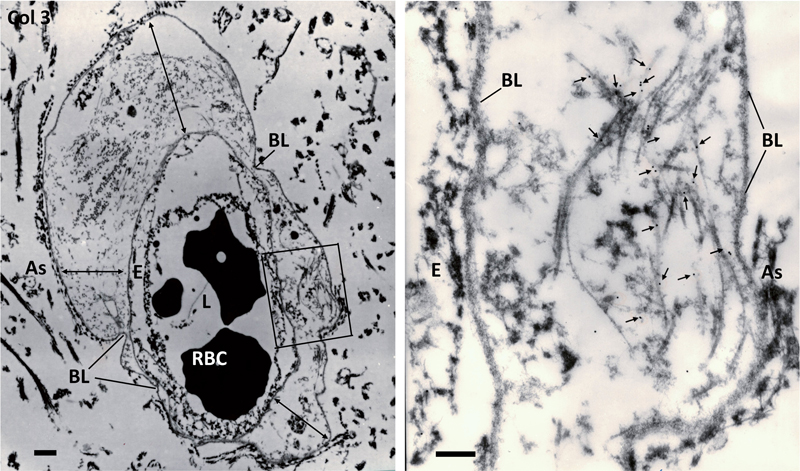
Fig 20. 46-year-old female with hereditary diffuse leukoencephalopathy with spheroids. Frontal cortex white matter. Immunogold electron micrographs of collagen type III (Col 3). Left. Cross section of a capillary showing fused basal laminas (BL) of endothelial cell (E) and perivascular astrocyte (As) splits and the resulting large and small expanded spaces [double head arrows] with deposits. RBC, red blood cell in capillary lumen (L). Right. Enlargement of boxed area reveals localization of Col 3 to longitudinal banded fibrils [arrows] in the expanded space, but not the split thin BL. Scale bars, left, 1 μm; right, 300 nm.
Fig 21. 46-year-old female with hereditary diffuse leukoencephalopathy with spheroids. Frontal cortex white matter. Immunogold electron micrographs of collagen type IV (Col 4). Left. Cross section of a capillary showing fused basal lamina (BL) of endothelial cell (E) and perivascular astrocyte (As) splits and the resulting large and small expanded spaces [double head arrows] with deposits. RBC, red blood cell in capillary lumen (L). Right. Enlargement of boxed area reveals localization of Col 4 to the split thin BL (arrows point to gold particles), but not banded fibrils [long arrows] in the expanded space.
Fig 22. 46-year-old female with hereditary diffuse leukoencephalopathy with spheroids. Frontal cortex white matter. Immunogold electron micrographs of fibronectin (FN). Left. Cross section of a capillary showing fused basal lamina (BL) of endothelial cell (E), pericyte [P] and perivascular astrocyte (As) splits and the resulting large and small expanded spaces [double head arrows] with deposits. L, capillary lumen; RBC, red blood cell. Right. Enlargement of boxed area reveals many gold particles [arrows] over banded fibrils and split thin BL. Immunoreactivity for Col 1 and Col 3 was localized to collagen fibrils, while Col 4 was mainly localized to the split BL and the normal appearing fused BL. Col 3 was more abundant than Col 1 in some cases, as seen on IHC. The reason for this differential immunoreactivity is not clear. It could be differential antibody reactivity, differential amount of collagen in the expanded space, or an age-related finding. Fibronectin was heavily localized to fibrils and BL where Col 6 was weakly localized. In normal or transgenic mice younger than 10 months (equivalent to 50 years of human age), the fused BL of the endothelial cell, pericyte and perivascular astrocytes did not split to form expanded spaces (Figs 23–28).
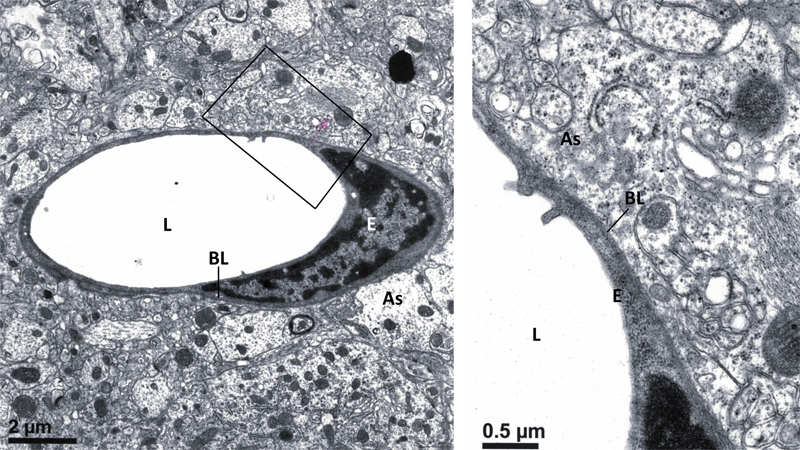
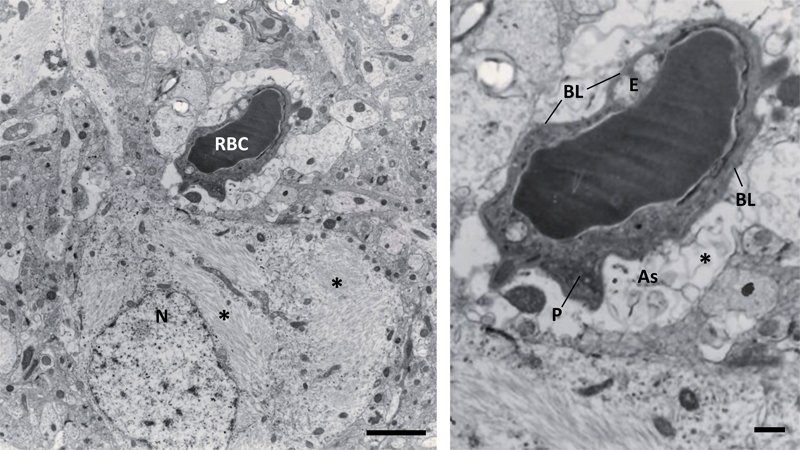
Fig 23. 1-month-old mouse (equivalent to 14-years-old human), expressing TAR DNA-binding protein 43 kD (TDP-43). Cortex. Left. A capillary is surrounded by fused basal lamina (BL) of endothelial cell (E) and perivascular astrocyte (As). Note the homogeneity and uniform thickness of amorphous BL. L, lumen. Right. Enlarged boxed area.
Fig 24. 2.5-months-old mice (equivalent to 22-years-old human). Globus pallidus. Left. normal. A capillary with a fused basal lamina [BL] of endothelial cell (E), pericyte (P) and perivascular astrocyte (As). Note the homogeneity and uniform thickness of amorphous BL. L, lumen. Right. drug-induced hepatic encephalopathy. Despite swelling of perivascular astrocyte (As), BL remains normal.
Fig 25. 5.5-months-old non-transgenic mouse (equivalent to 30-years-old human). Cortex. Two capillaries both have a fused basal lamina (BL) of endothelial cell (E), pericyte (P) and perivascular astrocyte (As). Note the homogeneity and uniform thickness of amorphous BL. RBC, red blood cell in the lumen (L); Ax, myelinated axon.
Fig 26. 5.5-month-old non-transgenic mouse (equivalent to 30-years-old human). Spinal cord. Top. Longitudinal section of a capillary showing fused basal lamina (BL) of endothelial cell (E), pericyte (P) and perivascular astrocyte (As). Bottom. Enlarged box areas. Note the homogeneity and uniform thickness of amorphous BL. L, capillary lumen; Ax, myelinated axon.
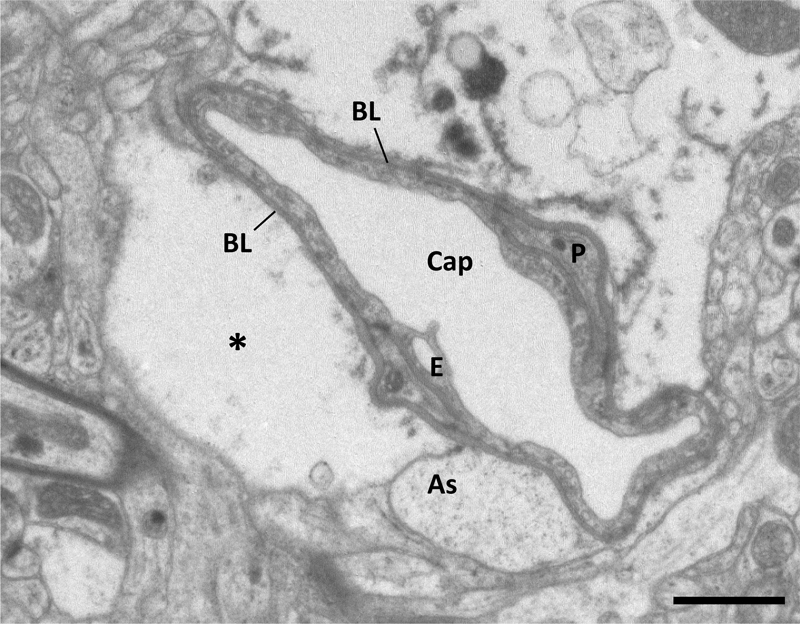
Fig 27. 7-months-old, transgenic mouse (equivalent to 38-years-old human) expressing C9orf72 mutation. Motor cortex. A capillary (Cap) with perivascular edema [*], but the fused basal lamina (BL) of endothelial cell (E), pericyte (P) and perivascular astrocyte (As) maintains amorphous homogeneity and uniform thickness. Scale bar, 1 μm.
Fig 28. 9-months-old, transgenic mouse (equivalent to 46-years-old human) expressing tau/amyloid precursor protein mutations. Cortex. Left. A red blood cell (RBC) fills the lumen of a capillary adjacent to a neuron [N] with heavy deposits of tau filaments [*]. Right. Enlargement of the capillary shows the fused basal lamina (BL) of endothelial cell (E), pericyte (P) and perivascular astrocyte (As) maintains its amorphous homogeneity and uniform thickness, despite edema around the vessel [*]. Scale bars, Left, 3 μm; right, 1 μm. Discussion Summary of major findings This study includes two aspects of capillary BL in human CNS that have long been ignored. The first being EM evidence of collagen fibrils in capillary BL in human CNS. We confirmed early findings and expanded upon our previous reports [25, 39] with IHC, EM and post-embedding IEM in a cohort of 45 patients ranging in age from 4 days to 49 years. The case number is relatively modest, but it includes a spectrum of CNS disorders, as well as those without significant brain pathology. In all cases, a similar morphologic observation was made, regardless of age, sex, disease, tissue region or PMI. The common findings included CNS microvessels that were IHC-positive for Col 1, Col 3, Col 4 and Col 6. EM studies revealed fused BL of endothelial cells, pericytes and perivascular astrocytes with focal splitting of the BL forming small to large spaces bordered by split BL and filled with fibrillar collagens, but no cellular components. No pericapillary space or astrogliosis was detected on the external BL. IEM showed localization of Col 1 and Col 3 in fibrils in the expanded spaces, but not the split BL. Non-fibrillar Col 4 was absent from expanded spaces, but was localized to the BL, including the split BL, which was not thickened or duplicated. Importantly, ultrastructural findings similar to those observed in humans were rarely detected in mouse brain and spinal cord. Evidence that the findings are genuine and not artifactual It is highly unlikely that the observed ultrastructural change in capillaries were due to postmortem changes. Previous investigators who have found similar results have argued that short PMI, uniform tissue handling/processing, as well as the inherent biochemical stability of collagen fibrils argues against these observations being artifactual [21–23, 26]. Although vascular cells produce fibrillar collagens, it is unlikely that the collagen fibrils that we observed are produced and deposited as a terminal event given that the PMI of most of the cases studied was short. Additionally, biopsy tissues in our cases, as well as in previous reports [34–36] argue against these being postmortem changes. Underrecognized features of human CNS capillaries It is not clear why capillary BL expansions with fibrillar collagen deposits have not been previously reported in humans. Several factors could explain the oversight. For one, there is a prevailing assumption that brain capillaries are the same in humans and mice, and comparative studies are rare. In addition, detailed studies on the ultrastructure of human microvasculature are few. Another factor to consider is that there may be variability in microvascular structures in different regions of the human brain. The cortical microvascular network is organized like a grid structure, while non-anastomotic vessels and capillary beds are common in the striatum [56, 57]. Neocortical regions are not equivalent and there are also differences related to aging and disease [58]. A recent study showed that human capillary endothelial cells from isolated microvessels from fresh brain tissue of fetuses,adult controls, and diseased brains had high transcriptional heterogeneity [59]. Since BL is produced by endothelial cells, it is possible that BL morphology is also heterogeneous. In this report we studied capillary BL of normal fetal and adult humans in cortical and subcortical gray matter and in cerebral white matter. In addition, we studied microvessels in a range of neurologic disorders in people younger than 50 years of age. Other investigators may not have such advantages. The main findings of this study are based on qualitative analysis by EM, which is a labor intensive procedure. Access to human samples, as well as limited EM resources and the time and effort involved in ultrastructural analysis may in part explain the paucity of similar studies in the scientific literature [9, 11]. Advances in microscopic techniques at the light microscopic level [60] could make comparative studies of microvessels in humans and animals more approachable. Additional comprehensive structural studies are needed to validate our findings and address their potential contribution to normal microvascular physiology and pathology. Evidence that the findings are not due to aging Our findings of extensive collagen fibril deposits in expanded BL spaces of young individuals argue against the observations being due to aging or specific disorders associated with BL pathology in human CNS capillaries [37, 53–55]. While detailed cardiovascular histories were not routinely recorded, chronic cardiovascular disease is uncommon at young ages. More studies of capillary BL from young people are needed to address this novel finding. Our ultrastructural observations are unlikely specific to a particular disease because they were found in a range of CNS disorders. Comparable findings in cases without significant brain pathologies further support the notion that capillary BL morphologies are characteristic of human CNS capillaries. Physiological implications of collagen deposition in blood vessels Collagens in extracellular matrix are now recognized as being more than an inert scaffold for mechanical support, instead they are thought to play an active role in homeostasis between vascular and perivascular elements [61]. The adult human brain has an extensive microvasculature for physiologic metabolic and energy demands, while these requirements are less in the mouse. Consequently, it is reasonable to expect more regulatory controls of blood flow in human CNS, even under normal physiological conditions, than in mice. Studies in both human and mouse brain show that the capillary bed has the highest resistance to blood flow within the cerebral vasculature [6, 62]. Blood flow regulation in capillaries has been studied in endothelial cells [63], pericytes [8] and astrocytes [64]. These cells are closely adherent to the capillary BL. Therefore, BL components may also have a role in blood flow control by their molecular interaction with vascular cells. Previous studies on brain vascular BL components frequently highlight Col 4 [9, 11, 65]; however, our recent study questioned the involvement of Col 4 in small vessel disease and in the hypertensive rat [66]. The IHC findings in this report show Col 4 in BL of capillary endothelial cells and the split pericapillary BL, but not in the space produced by the BL splitting. IEM further confirmed the absence of Col 4 in expanded BL spaces. This, plus the absence of remodeling in the split BL in capillaries of normal and pathological brain samples, suggests that Col 4 has a minimal role in producing this unique capillary structure, which is found even in young individuals less than 50 years of age. An in vitro study of contractile cells grown on experimental matrix composed of Col 1 responded to strain/deformation faster than on Matrigel (mouse sarcoma derived matrix containing 30 % Col 4, 60 % laminin, and 8 % entactin) suggesting cells grown on Col 1-matrix could communicate mechanical information to other cells over considerable distances (67). We propose that in addition to other BL components, fibrillar Col 1 and Col 3 might provide an extra control mechanism to regulate capillary blood flow related to their inherent tensile and elastic properties. Functions of collagens in human capillary basal lamina in pathological conditions Structural defects of Col 1 and Col 3 are thought to contribute to vascular wall fragility in disorders such as Ehlers-Danlos syndrome [68]. On the other hand, increased Col 1 and Col 3 in media of arterioles and pericapillary spaces of subcortical white matter is characteristic of Binswanger’s disease [69, 70]. It has been suggested that fibrillar collagens strengthen the vascular wall in response to degeneration in the media in familial and sporadic arteriosclerotic disorders. In human cystic fibrosis, damage to the lung epithelial barrier will allow protease such as matrix metalloproteases (MMP) and prolyl endopeptidase to reach and digest the underlying matrix containing Col 1. The ensuing collagen fragments then act as a neutrophile chemoattractant in chronic inflammation [71]. It has been shown that MMP-9 can degrade native Col 1 and Col 3 [72], and increased expression or activity of MMP is known in neurodegenerative diseases [73]. Our data showed abundant Col 1 and Col 3 fibrils in the expanded spaces in human brain capillary BL. In a similar scenario to lung epithelial barrier breakdown, these collagens could be targeted by proteases that breach the BBB, leading to fragment peptides that are involved in inflammation during neurodegeneration. Col 1 binds within residues 448–465 of amyloid protein precursor protein (APP-695) [74]. APP was previously shown to trigger activation of monocytes upon adhesion to Col 1, which typically occurs during adhesion of monocytes to vascular endothelium or during tissue infiltration by monocyte/macrophages [74]. Interestingly, a recent report of amyloid immunotherapy in the PDAPP mouse model of AD showed upregulated protein levels of MMT 9 by activated perivascular macrophages [76]. This may be related to the pathogenesis of amyloid-related imaging abnormalities (ARIA) in certain AD patients after immunotherapies [77]. Also, macrophages could phagocytize drugs that pass the BBB and prevent them from reaching their target cell. Species specify of observed findings Our data is the first to show ultrastructural difference between human and mouse CSF capillary BL, with prevailing presence of fibrillar Col 1 and Col 3 and minimal involvement of Col 4. The expanded spaces in BL containing fibrillar collagens were observed in human CNS even at lower magnifications, but similar structures are not observed in even old mice. The large, expanded spaces with fibrillar collagen deposits are not found in adult mice (up to 10 months of age in this study and 2 years of age in an unpublished study). Rarely, a few fibrillar collagens fibrils are found in BL at higher magnifications. If these expanded BL spaces were a common feature in capillaries of mouse CNS, it is unlikely previous EM studies would have missed them. Two recent studies of brain capillary BL in young and aged mice, as well as early studies of spinal cord capillaries in ALS mouse models, showed thickened BL, but no fibrillar collagens [78–81]. Mouse models of human diseases are valuable tools for new avenues of research and therapy development; however, species differences between humans and mice have been noted [82]. Furthermore, translational data from mouse models to humans does not always succeed, including in neurodegenerative disorders/diseases [83–85]. The implication of species differences, if any, remains to be elucidated. Recent genomic studies showed species differences between human and mouse cortical neurons and glial cells [86], as well as differences in recent transcriptomic analyses of human and mouse brain vascular cells [16–18, 58, 59, 87]. Future studies need to address the role of specific collagens, given the recent report showing difference in expression of COL3A1 gene in mouse and human lung [88]. In conclusion, our data showed that, in the human CNS, capillary BL contains fibrillar Col 1 and Col 3 in expanded spaces formed by splitting of the BL that are not found in mouse CNS. We suggest that in human CNS capillary BL, a “Col 4-centric” dogma needs to be modified to include fibrillar collagens, in particular Col 1 and Col 3. Aspects of CNS vascular biology in humans has been inferred from mouse studies, but these results may need to be revised. Additional studies that focus on unique capillary BL structure and the functional significance of fibrillary collagens in human CNS in physiology and pathology are needed. Acknowledgements We are grateful to the tissue donors and their families. We thank Virginia Phillips, Monica Castanedes-Casey, Nathan Perez, and Whitney Davis for their assistance in histology and immunohistochemistry. Conflict of interest statement The authors declare no conflict of interests. Funding statement Funded by NIH grants and Mayo Foundation. Supplementary material References 1. Fawcett DW. A textbook of Histology. Philadelphia PA: WB Saunders Company 1986. https://archive.org/details/textbookofhistol0011fawc 2. Bär T, Wolff JR. The formation of capillary basement membranes during internal vascularization of the rat’s cerebral cortex. Z Zellforsch 1972;133:231–248. https://doi.org/10.1007/BF00307145 3. Hauw J-J, Berger B, Escourolle R. Electron microscopic study of the developing capillaries of human brain. Acta Neuropathol 1975;229–242. https://doi.org/10.1007/BF00684562 4. Marίn-Padilla M. The human brain intracerebral microvascular system: development and structure. Front Neuroanat 2012;6:38. https://doi.org/10.3389/fnana.2012.00038 5. Sweeney MD, Zhao Z, Montagne A et al. Blood-brain-barrier: from physiology to disease and back. Physiol Rev 2019;99:21–78. https://doi.org/10.1152/physrev.00050.2017 6. Gould IG, Tsai P, Kleinfeld D et al. The capillary bed offers the largest hemodynamic resistance to the cortical blood supply. J Cereb Blood Flow Metab 2017;37:52–68. https://doi.org/10.1177/0271678X16671146 7. Armulik A, Genove G, Mae M et al. Pericytes regulate the blood-brain barrier. Nature 2010;468:557–561. https://doi.org/10.1038/nature09522 8. Longden TA, Zhao G, Hariharan A et al. Pericytes and the control of blood flow in brain and heart. Ann Rev Physiol 2023;85:137–164. https://doi.org/10.1146/annurev-physiol-031522-034807 9. Thomsen MS, Routhe LJ, Moos T. The vascular basement membrane in the healthy and pathological brain. J Cereb Blood Flow Metab 2017;37:3300–3317. https://doi.org/10.1177/0271678X17722436 10. Mastorakos P, McGavern D. The anatomy and immunology of vasculature in the central nervous system. Sci Immunol 2019;4:eaavo492. https://doi.org/10.1126/sciimmunol.aav0492 11. Nguyen B, Bix G, Yao Y. Basal lamina changes in neurodegenerative disorders. Mol Neurodegen 2021;16:81. https://doi.org/10.1186/s13024-021-00502-y 12. Martinez-Hernandez A, Amenta PS. The basement membrane in pathology. Lab Invest 1983;48:656–677. https://pubmed.ncbi.nlm.nih.gov/6222217/ 13. Nirwane A, Yao Y. Cell-specific expression and function of laminin at the neurovascular unit. J Cereb Blood Flow Metab 2022;42:1979–1999. https://doi.org/10.1177/0271678X221113027 14. Dempsey EW, Wislocki GB. An electron microscopic study of the blood-brain barrier in the rat, employing silver nitrate as a vital stain. J Biophys Biochem Cytol 1955;1:245–256. https://doi.org/10.1083/jcb.1.3.245 15. Muldoon LL, Pagel MA, Kroll RA, et al. A physiological barrier distal to the anatomical blood-brain barrier in a model of transvascular delivery. Am J Neuroradiol 1999;20:217–222. https://pmc.ncbi.nlm.nih.gov/articles/PMC7056106/ 16. Zhang Y, Sloan SA, Clarke LE et al. Purification and characterization of progenitor and mature human astrocytes reveals transcriptional and functional differences with mouse. Neuron 2016;89:37–53. https://doi.org/10.1016/j.neuron.2015.11.013 17. Song HW, Foreman KL, Gastfriend BD et al. Transcriptomic comparison of human and mouse brain microvessels. Sci Rep 2020;19:12358. https://doi.org/10.1038/s41598-020-69096-7. 18. Ulbrich P, Khoshneviszadeh M, Jandke S et al. Interplay between perivascular and perineuronal extracellular matrix remodeling in neurological and psychiatric diseases. Eur J Neurosci 2021;53:3811–3830. https://doi.org/10.1111/ejn.14887 19. Garcia FJ, Sun N, Lee H et al. Single-cell dissection of the human brain vasculature. Nature 2022;603:893–899. https://doi.org/10.1038/s41586-022-04521-7 20. Yang AC, Vest RT, Kern F et al. A human brain vascular atlas reveals diverse mediators of Alzheimer’s risk. Nature 2022;603:885–892. https://doi.org/10.1038/s41586-021-04369-3 21. Cervόs-Navaro J, Ferszt R. Connective tissue in pericapillary spaces of the human spinal cord. Acta Neuropathol 1973;24:178–183. https://doi.org/10.1007/BF00684839 22. Ferszt R, Cervós-Navarro J, Sasaki S. Pericapillary spaces in the human spinal cord. In: Cervós-Navarro J, ed. Pathology of Cerebral Circulation. Berlin: Walter de Gruyter 1974:59–66. https://doi.org/10.1515/9783111506852-008 23. Ono S, Imai T, Munakata S et al. Collagen abnormalities in the spinal cord from patients with amyotrophic lateral sclerosis. J Neurol Sci 1998;160:140–147. https://doi.org/10.1016/s0022-510x(98)00223-8 24. Garbuzova-Davis S, Hernandez-Ontiveros DG, Roderigues MCO, et al. Impaired blood-brain/spinal cord barrier in ALS patients. Brain Res 2012;1469:114–128. https://doi.org/10.1016/j.brainres.2012.05.056 25. Lin W-L, Dickson DW. Distinct ultrastructural characteristics of capillary basal lamina in human and mouse brains: relevance to murine models of neurovascular disease. (Abstract). Alzheimer’s & Dementia 2017;13 [Sup]:1391–1392. https://doi.org/10.1016/j.jalz.2017.06.2147 26. Sasaki S. Alterations of the blood-spinal cord barrier in sporadic amyotrophic lateral sclerosis. Neuropathology 2015;35:518–528. https://doi.org/10.1111/neup.12221 27. Wiśniewski HM, Coblentz JM, Terry RD. Pick’s disease. A clinical and ultrastructural study. Arch Neurol 1972;26:97–108. https://doi.org/10.1001/archneur.1972.00490080015001 28. Weller RO, Griffin RL. Transmission and scanning electron microscopy of the microcirculation of gliomas. Adv Neurol 1978;20:569-575. PMID: 676920https://pubmed.ncbi.nlm.nih.gov/676920/ 29. Allsopp G, Gamble HJ. An electron microscopic study of the pericytes of the developing capillaries in human fetal brain and muscle. J Anat 1979a;128:155-168. PMID: 422476https://pubmed.ncbi.nlm.nih.gov/422476/ 30. Allsopp G, Gamble HJ. Light and electron microscopic observations on the development of the blood vascular system of the human brain. J Anat 1979b;128:461-477. PMCID: PMC1232901https://pmc.ncbi.nlm.nih.gov/articles/PMC1232901/ 31. Mancardi GL, Perdelli F, Rivano C et al. Thickening of basement membrane of cortical capillaries in Alzheimer’s disease. Acta Neuropathol 1980;49:79–83. https://doi.org/10.1007/BF00692225 32. Ferszt R, Cervós-Navarro J. Cerebrovascular pathology- aging and brain failure. In: Cervós-Navarro J, Sarkander H-I, eds. Brain Aging: Neuropathology and Neuropharmacology, Aging vol 21, Raven Press, New York, 1983:133–151. https://doi.org/10.1093/jnen/43.2.213 33. Shibata S. Ultrastructure of capillary walls in human brain tumors. Acta Neuropathol 1989;78:561–571. https://doi.org/10.1007/BF00691283 34. Castejón OJ. Electron microscopic study of capillary wall in human cerebral edema. J Neuropath Exp Neurol 1980;39:296–328. https://doi.org/10.1097/00005072-198005000-00006 35. Claudio L, Raine CS, Brosnan CF. Evidence of persistent blood-brain barrier abnormalities in chronic-progressive multiple sclerosis. Acta Neuropathol 1995;90:228–238. https://doi.org/10.1007/BF00296505 36. Claudio L. Ultrastructural features of the blood-brain barrier in biopsy tissue from Alzheimer’s disease patients. Acta Neuropathol 1996;91:6–14. https://doi.org/10.1007/s004010050386 37. Farkas E, de Vos RAI, Donka G et al. Age-related microvascular degeneration in the human cerebral periventricular white mater. Acta Neuropathol 2006:111:150–157. https://doi.org/10.1007/s00401-005-0007-y 38. Szpak GM, Lewandowska E, Wierzba-Bobrowicz t et al. Small cerebral vessel disease in familial amyloid and non-amyloid angiopathies: FAD-PS-1 [P117L] mutation and CADASIL immunohistochemical and ultrastructural studies. Folia Neuropathol 2007;45:192–204. https://pubmed.ncbi.nlm.nih.gov/18176893/ 39. Lin W-L, Castanedes-Casey M, Dickson DW. Ultrastructural analysis of capillary basal lamina components in amyotrophic lateral scleroses. (Abstract). J Neuropathol Exp Neurol 2013;72:554–555. https://doi.org/10.1097/NEN.0b013e318299610e 40. van Duinen SG, Maat-Schieman MLC, Bruijn JA et al. Cortical tissue of patients with hereditary cerebral hemorrhage with amyloidosis [Dutch] contains various extracellular matrix deposits. Lab Invest 1995;73:183–189. https://pubmed.ncbi.nlm.nih.gov/7637318/ 41. Dong H, Blaivas M, Wang MM. Bidirectional encroachment of collagen into the tunica media in cerebral autosomal dominant arteriopathy with subcortical infracts and leukoencephalopathy. Brain Res 2012;1456:64–71. https://doi.org/10.1016/j.brainres.2012.03.037 42. Hondius DC, Eigenhuis KN, Morrema THJ et al. Proteomics analysis identifies new markers associated with capillary cerebral amyloid angiopathy in Alzheimer’s disease. Acta Neuropathol Commun 2018;6:46. https://doi.org/10.1186/s40478-018-0540-2 43. Ojo JO, Reed JM, Crynen G et al. Molecular pathobiology of the cerebrovasculature in aging and in Alzheimers disease cases with cerebral amyloid angiopathy. Front Aging Neurosci 2021;13:1–13. https://doi.org/10.3389/fnagi.2021.658605 44. Endo Y, Hasegawa K, Nomura R et al. Apolipoprotein E and clusterin inhibit early phase of amyloid-β aggregation in an in vitro model of cerebral amyloid angiopathy. Acta Neuropathol Commun 2019;7:12. https://doi.org/10.1186/s40478-019-0662-1 45. Hou Y, Dan X, Babbar M, et al. Ageing as a risk factor for neurodegenerative disease. Nat Rev Neurol 2019;15:565–581. https://doi.org/10.1038/s41582-019-0244-7 46. Chen R-L, Balami JS, Esiri MM et al. Ischemic stroke in the elderly: an overview of evidence. Nat Rev Neurol 2010;6:256–265.. https://doi.org/10.1038/nrneurol.2010.36 47. Degl’Innocenti E, Dell’Anno MT. Human and mouse cortical astrocytes: a comparative view from development to morphological and functional characterization. Front Neuroanat 2023;. https://doi.org/10.3389/fnana.2023.1130729 48. Lewis J, McGowan E, Rockwood J et al. Neurofibrillary tangles, amyotrophy and progressive motor disturbance in mice expressing mutant [P301L] tau protein. Nat Genet 2000;25:402–405. https://doi.org/10.1038/78078 49. Xu Y-F, Zhang Y-J, Lin W-L, et al Expression of mutant TDP-43 induces neuronal dysfunction in transgenic mice. Mol Neurodegen 2011;6:73. https://doi.org/10.1186/1750-1326-6-73 50. Chew J, Gendron TF, Prudencio M et al. C9ORF72 repeat expansions in mice cause TDP-43 pathology, neuronal loss, and behavioral deficits. Science 2015;348:1151–1154. https://doi.org/10.1126/science.aaa9344 51. Uchikado H, Lin W-L, DeLucia MW et al. Alzheimer disease with amygdala Lewy bodies: a distinct form of α-synucleinopathy. J Neuropathol Exp Neurol 2006;65:685–697. https://doi.org/10.1097/01.jnen.0000225908.90052.07 52. Matsunaga T, Kanzaki J, Hosoda Y. Ultrastructure of astrocytes in transitional region of human eight cranial nerve. Hearing Res 1994;76:118–126. https://doi.org/10.1016/0378-5955(94)90093-0 53. De Jong GI, de Vos RAI, Jansen Steur ENH et al. Cerebrovascular hyperperfusion: a risk factor for Alzheimer’s disease? Animal model and postmortem human studies. Ann New York Acad Sci 1997;826:56–74. https://doi.org/10.1111/j.1749-6632.1997.tb48461.x 54. Farkas E, De Jong GI, Apró E et al. Similar ultrastructural breakdown of cerebral capillaries in Alzheimer’s disease, Parkinson’s disease, and Experimental Hypertension. What is the functional link? Ann New York Acad Sci 2000;903;72–82. https://doi.org/10.1111/j.1749-6632.2000.tb06352.x 55. Farkas E, Luiten PGM. Cerebral microvascular pathology in aging and Alzheimer’s disease. Prog Neurobio 2001;64:575–611. https://doi.org/10.1016/s0301-0082(00)00068-x 56. Feekes JA, Cassell MD. The vascular supply of the functional compartments of the human striatum. Brain 2006;129:2189–2201. https://doi.org/10.1093/brain/awl158 57. Schmid F, Barrett MJP, Jenny P et al. Vascular density and distribution in neocortex. NeuroImage 2019;197;792–805. https://doi.org/10.1016/j.neuroimage.2017.06.046 58. Bryant A, Li Z, Jayakumar R et al. Endothelial cells are heterogeneous in different brain regions and are dramatically altered in Alzheimer’s disease. J Neurosci 2023;43:4541–4557. https://doi.org/10.1523/JNEUROSCI.0237-23.2023 59. Wälchli T, Ghobrial M, Schwab M et al. Single-cell atlas of the human brain vasculature across development, adulthood and disease. Nature 2024;632:603–613. https://doi.org/10.1038/s41586-024-07493-y 60. Shahidehpour RK, Nelson PT, Bachstetter AD. A pathologic study of perivascular pTDP-43 Lin bodies in LATE-NC. Acta Neuropathol Commun 2024;12:114. https://doi.org/10.1186/s40478-024-01826-8 61. Wareham LK, Baratta RO, Del Buono BJ et al. Collagen in the central nervous system: contributions to neurodegeneration and promise as a therapeutic target. Mol Neurodegen 2024; 19:11.. https://doi.org/10.1186/s13024-024-00704-0 62. Linninger AA, Gould IG, Marinnan T et al. Cerebral microcirculation and oxygen tension in the human secondary cortex. Ann Biomed Eng 2013; 41:2264–2284. https://doi.org/10.1007/s10439-013-0828-0 63. Sargent SM, Bonney SK, Li Y et al. Endothelial structure contributes to heterogeneity in brain capillary diameter. Vasc Biol 2023;5:e230010. https://doi.org/10.1530/VB-23-0010 64. Metea MR, Newman EA. Glial cells dilate and constrict blood vessels: a mechanism of neurovascular coupling. J Neurosci 2006;26:2862–2870. https://doi.org/10.1523/JNEUROSCI.4048-05.2006 65. Howe MD, McCullough LD, Urayama A. The role of basement membrane in cerebral amyloid angiopathy. Front Physiol 2020;11:601320. https://doi.org/10.3389/fphys.2020.601320 66. Kumar CM, Yeo N, Whittaker M et al. Vascular collagen-IV in hypertension and cerebral small vessels disease. Stroke 2022;53:3696–3705. https://doi.org/10.1161/STROKEAHA.122.037761 67. Miller RT. Mechanical properties of basement membrane in health and disease. Matrix Biol 2017;57–58:366–373. https://doi.org/10.1016/j.matbio.2016.07.001 68. Malfait F. Vascular aspects of the Ehlers-Danlos syndromes. Matrix Biol 2018:71–71:380–395. https://doi.org/10.1016/j.matbio.2018.04.013 69. Zhang WW, Olsson Y. The angiopathy of subcortical arteriosclerotic encephalopathy [Binswanger’s disease]: immunohistochemical studies using markers for components of extracellular matrix, smooth muscle actin and endothelial cells. Acta Neuropathol 1997;93;219–224. https://doi.org/10.1007/s004010050607 70. Lin J-X, Tomimoto H, Akiguchi I et al. Vascular cell components of the medullary arteries in Binswanger’s disease brains. A morphometric and immunoelectron microscopic study. Stroke 2000;31:1838–1842. https://doi.org/10.1161/01.str.31.8.1838 71. Gaggar A, Jackson PL, Noerager BD et al. A novel proteolytic cascade generates an extracellular matrix-derived chemoattractant in chronic neutrophilic inflammation. J Immunol 2008;180:5662–5669. https://doi.org/10.4049/jimmunol.180.8.5662 72. Bigg HF, Rowan AD, Barker MD, Cawston TE. Activity of matrix metalloproteinase-9 against native collet type I and III. FASEB J 2007;274:1246–1255. https://doi.org/10.1111/j.1742-4658.2007.05669.x 73. Behl T, Kaur G, Sehgal A et al. Multifaceted role of matrix metalloproteinases in neurodegenerative diseases: pathophysiological and therapeutic perspectives. Int J Mol Sci 2021;22:1413. https://doi.org/10.3390/ijms22031413 74. Beher D, Hesse L, Masters CL et al. Regulation of amyloid protein precursor [APP] binding to collagen and mapping of the binding sites on APP and collagen type I. J Biol Chem 1996;271:1613–1620. https://doi.org/10.1074/jbc.271.3.1613 75. Sondag CM, Combs CK. Adhesion of monocytes to type I collagen stimulates an APP-dependent proinflammatory signaling response and release of Aβ1-40. J Neuroinflammation 2010;7:22. https://doi.org/10.1186/1742-2094-7-22 76. Taylor X, Clark IM, Fitzgerald GJ et al. Amyloid-β [Aβ] immunotherapy induced microhemorrhages are associated with activated perivascular macrophages and peripheral monocyte recruitment in Alzheimer's disease mice. Mol Neurodegener 2023;18:59. https://doi.org/10.1186/s13024-023-00649-w 77. Sperling RA, Jack CR Jr, Black SE et al. Amyloid-related imaging abnormalities in amyloid-modifying therapeutic trials: recommendations from the Alzheimer’s Association Research Roundtable Workgroup. Alzheimers Dement 2011;7:367–385. https://doi.org/10.1016/j.jalz.2011.05.2351 78. Zhong Z, Deane R, Ali Z et al. ALS-causing SOD-1 mutants generate vascular changes prior to motor neuron degeneration. Nat Neurosci 2008;11:420–422. https://doi.org/10.1038/nn2073 79. Garbuzova-Davis S, Haller E, Saporta S et al. Ultrastructure of blood-brain barrier and blood-spinal cord barrier in SOD1 mice modeling ALS. Brain Res 2007;1157:126–137. https://doi.org/10.1016/j.brainres.2007.04.044 80. Ceafalan LC, Fertig TE, Gheorghe TC et al. Age-related ultrastructural changes of the basement membrane in the mouse blood-brain barrier. J Cell Mol Med 2019;23:819–827. https://doi.org/10.1111/jcmm.13980 81. Li C, Chen S, Siedhoff HR, et al. Low-intensity open-field blast exposure effects on neurovascular unit ultrastructure in mice. Acta Neuropathol Commun 2023;11:144. https://doi.org/10.1186/s40478-023-01636-4 82. Perlman RL. Mouse models of human disease. An evolutionary perspective. Evol Med Public Health. 2016:170–176. https://doi.org/10.1093/emph/eow014 83. VandeVrede L, La Joie R, Horiki S et al. Co-pathology may impact outcomes of amyloid-targeting treatments: clinicopathological results from two patients treated with aducanumab. Acta Neuropathol 2023;146:777–781. https://doi.org/10.1007/s00401-023-02631-8 84. Reish NJ, Jamshidi P, Stamm B et al. Multiple cerebral hemorrhages in a patient receiving Lecanemab and treated with t-PA for stroke. N Engl J Med 2023;388:478–479. https://doi.org/10.1056/NEJMc2215148 85. Genge A, Wainwright S, Vande Velde C. Amyotrophic lateral sclerosis: exploring pathophysiology in the context of treatment. Amyotroph Lateral Scler Frontotemporal Degener 2024;25:225–236. https://doi.org/10.1080/21678421.2023.2278503 86. Hodge RD, Bakken TE, Miller JA et al. Conserved cell types with divergent features in human versus mouse cortex. Nature 2019;573:61–68.. https://doi.org/10.1038/s41586-019-1506-7 87. Ihara M, Yamamoto Y. Transcriptomic mapping of the human cerebrovasculature. Nat Rev Neurol 2022;18;319–320. https://doi.org/10.1038/s41582-022-00650-9 88. Wang L, Liu H, Jiao Y et al. Differences between mice and humans in regulation and the molecular network of collagen type III, alpha-1 at the gene expression level: obstacles that translational research must overcome. Int J Mol Sci 2015;16:15031–15056. https://doi.org/10.3390/ijms160715031
Copyright: © 2025 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |