|
|
|
Free Neuropathology 6:5 (2025) |
|
Letter |
|
A novel KDM2A::YAP1 fusion in a pediatric supratentorial CNS neoplasm resembling a tumor with BCOR internal tandem duplication |
|
Arnault Tauziède-Espariat 1,2 , Alice Métais 1,2 , Dorian Bochaton 1 , Euphrasie Servant 1 , Guillaume Chotard 3 , Mégane Le Quang 3 , Benjamin Bonhomme 4 , Nathalène Truffaux 4 , Volodia Dangouloff-Ros 5 , Nathalie Boddaert 5 , Lauren Hasty 1 , Edouard Gimbert 6 , Pascale Varlet 1,2 on behalf of the RENOCLIP-LOC |
|
|
Corresponding author:
|
|
Additional resources and electronic supplementary material: supplementary material |
|
Submitted: 12 December 2024
|
|
Keywords: YAP1, KDM2A, BCOR, Tumor of the central nervous system |
|
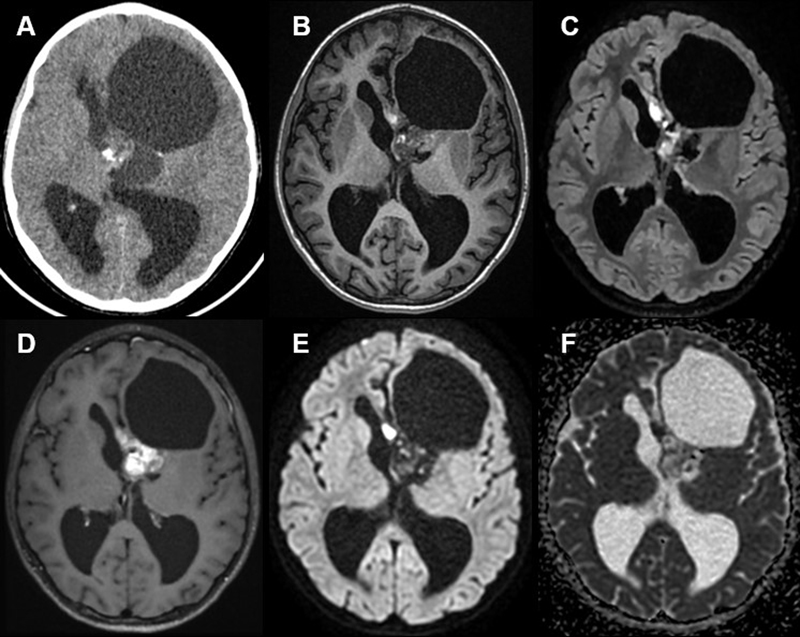
Introduction The central nervous system (CNS) tumor with BCOR internal tandem duplication (ITD), initially named high-grade neuroepithelial tumor (HGNET), was introduced as a novel embryonal neoplasm in the last World Health Organization (WHO) Classification of CNS tumors and in the German Cancer Research Center (Deutsches Krebsforschungszentrum, DKFZ) classifier as a distinct methylation class (1,2). Since its initial description, other alterations of BCOR and its ligand BCORL1 have been reported in CNS tumors having similar histopathological features. Among them, the fusion EP300::BCOR was evidenced in several cases with a distinct methylation class (3,4). Moreover, CNS tumors harboring fusions implicating other genes of the complex polycomb repressive complex 1.1 (PRC1.1) (KDM2B and NUTM2A/B genes) have been described (5). Herein, we report a brain neoplasm presenting the histopathological features of a CNS tumor with BCOR ITD, but harboring a KDM2A::YAP1 fusion. Case presentation A 10-year-old boy presented with intracranial hypertension, found to be caused by a supratentorial (ST) intraventricular neoplasm. Magnetic resonance imaging (MRI) revealed a large mass within the left lateral ventricle having solid and cystic content (MRI performed after cyst aspiration) (Figure 1B–F). Computerized tomography (CT) showed the solid component to have intermediate density and calcification (Figure 1A), intense contrast enhancement (Figure 1D), and no diffusion restriction (Figure 1E). The tumor was subtotally resected. Morphologically, this tumor was mainly well-circumscribed from the brain parenchyma (with few infiltrating isolated cells around the periphery of the tumor). Pseudorosettes, microcysts and calcifications were observed (Figure 2A–B). There was no necrosis or microvascular proliferation, but the tumor presented a high mitotic count (6 mitoses per 5 high-power fields representing 1.6 mm2) and proliferation index (10 %). Immunohistochemistry (IHC) confirmed the preserved expression of H3K27me3, INI1 and ATRX. There was no immunopositivity for GFAP, OLIG2 or MN1, and the expression of EMA was cytoplasmic without dot-like or microlumen staining. NeuN and neurofilament were expressed by a subset of tumor cells, and nuclear translocation of β-catenin was present. There was a weak, but diffuse, immunoreactivity for BCOR (Figure 2C) and a focal positivity for SATB2 (Figure 2D). RNA sequencing evidenced a KDM2A::YAP1 gene fusion (Figure 2E). Next-generation sequencing failed to reveal any other alteration. The tumor was not classifiable using the Heidelberg Brain Tumor and sarcoma (v12.8) or Bethesda Classifiers, nor by t-Distributed Stochastic Neighbor Embedding (t-SNE) or Uniform Manifold Approximation and Projection (UMAP) analyses (supplementary Figure 1), which included HGNET-BCOR and sarcomas with BCOR alterations and CNS and soft tissue tumors with YWHAE:NUTM2 or KDM2B fusions from our in-house database and previously reported (5). Forty-two months later, the patient presented a local recurrence of the tumor and a second surgery was performed. The recurrence histopathology was identical to the initial resection. The patient is alive without residue 60 months after the initial diagnosis and without any adjuvant treatment. Figure 1: Radiological features
Axial unenhanced CT(A), T1-weighted (B), FLAIR (C), post-contrast T1-weighted (D), diffusion (E), and apparent diffusion coefficient (ADC) map (F) images of the patient, showing a large mass within the left lateral ventricle having solid and cystic content (MRI performed after cyst aspiration). CT showed the solid component to have intermediate density and calcification, intense contrast enhancement, and no diffusion restriction. Figure 2: Histological and molecular features
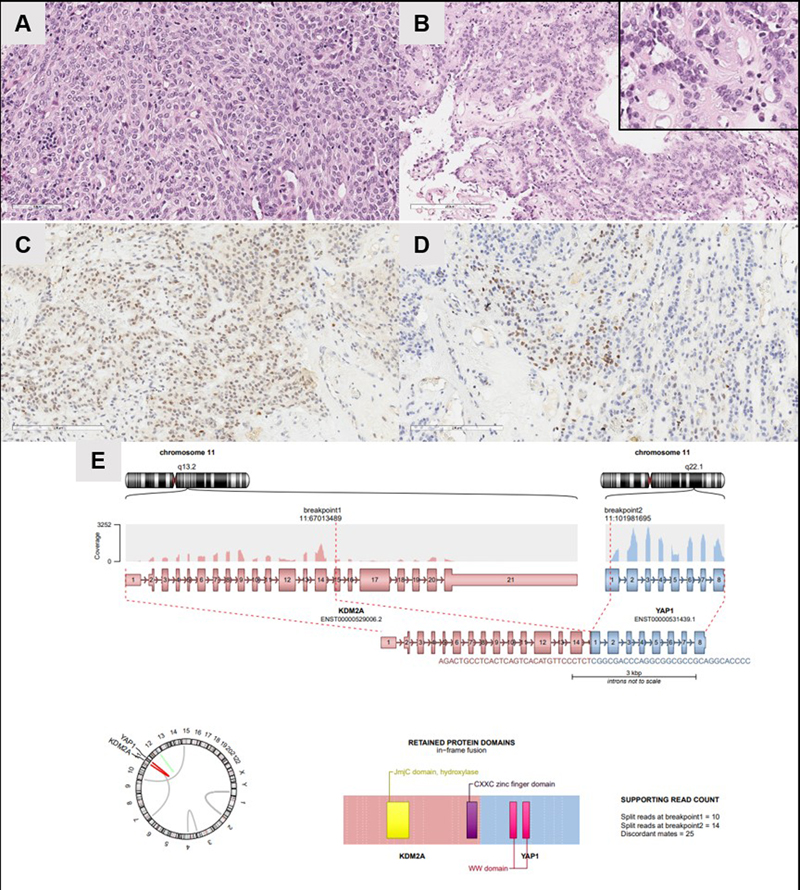
The tumor was solid and composed of uniform oval or spindle-shaped cells with round to oval nuclei, a dense capillary network (A,Hematoxylin phloxin saffron (HPS), magnification x400), pseudorosettes and microcystic formations (B, HPS, magnification x400). BCOR protein immunoreactivity was weak in the tumor cells (C, magnification x400). Expression of SATB2 in a subset of tumor cells (D, magnification x400). E RNA-sequencing analysis evidenced a KDM2A::YAP1 fusion. Discussion and conclusions In the Heidelberg classifier (v12.8), two distinct methylation classes of CNS tumors characterized by different BCOR alterations exist: CNS tumors with BCOR ITD and those with EP300::BCOR fusion, with only the first being part of the current WHO classification (2). Regarding data from the literature (n = 82), CNS tumors with BCOR ITD affect mainly children (95 % of reported cases are pediatric with a median age of 3.5 years-old) and are distributed supratentorially and infratentorially (58 % and 42 % of reported cases, respectively) with a poor outcome (37 % patients were dead with a median overall survival of 20 months) (6–20). Contrarily, CNS tumors with an EP300:BCOR fusion (n = 24) concern young adults (median age of 28 years-old), are mostly supratentorial (83 % of reported cases) and seem to be associated with a better prognosis (no death reported to date in the literature and a median overall survival of 16 months) (3,4,16). Whereas CNS tumors with a EP300::BCOR fusion can present a broad histological spectrum (4), these two molecular entities may share similar histopathological features: a predominantly solid growth pattern, uniform oval or spindle-shaped cells with round to oval nuclei, a dense capillary network, and pseudorosette formations (3). Because of the nature of the antibody, only tumors with BCOR ITD showed a constant overexpression of the BCOR protein using IHC (4,21). In the literature, other alterations implicating the BCOR gene (CREBBP::BCOR fusions) or its ligand BCORL1 (EP300::BCORL1, CREBBP::BCORL1 fusions) have been reported (16,22,23), for which SATB2 IHC may constitute a helpful diagnostic tool, being positive in CNS tumors with BCOR alterations (regardless of their molecular abnormality), and in sarcoma harboring KDM2B or YWHAE fusions (1,2). The current case showed a focal positivity for this antibody. Interestingly, this case along with other rare CNS tumors and soft tissue/visceral sarcomas which have been found to harbor classically BCOR alterations, have been shown to have KDM2A or KDM2B fusions (5,24,25). Associated with BCOR in the PRC1.1 complex, KDM2A and B (Lysine Demethylase 2A and B) proteins mediate the transcriptional repression of tumor suppressors through the post-translational modifications of histones. The predicted fusion protein of the current case maintained major functional domains, such as the jumonji C and CXXC DNA-binding domains of the KDM2A gene and the WW domain of the YAP1 gene which is a transcriptional co-activator as previously described (2,5). YAP1 fusions are well known in the tumorigenesis of ependymomas (EPN) and it has been evidenced that they are sufficient to form tumors in the developing mouse brain (3). Moreover, the overexpression of the YAP1 protein in cortical progenitor cells induces an activation of the Hippo pathway and is implicated in cell proliferation (3). In contrast to previously reported CNS cases harboring an alternative gene fusion of the PRC1.1 complex, the current tumor presented histopathological similarities to CNS tumors with BCOR alterations but not sarcomas (5). However, the DNA-methylation analysis did not permit its classification. This is potentially due to the fact that only CNS tumors with BCOR alterations are present in the current classifier and that the boundaries of the current methylation classes are not clearly defined, with a subset of cases being misclassified (4,22). Other samples having these rare alterations are necessary to determine if they cluster together and form a distinct methylation class from those described. In closing, we report herein a CNS tumor having histopathological similarities to CNS tumors with BCOR alterations, but having a fusion implicating the gene KDM2A, encoding a protein of the PRC1.1 complex. In cases of a suspected CNS tumor with BCOR alteration without a strong and diffuse immunopositivity for the BCOR protein, RNA-sequencing analysis may help to diagnose alternative fusions. Ethics approval This study was approved by GHU Paris - Psychiatry and Neuroscience, Sainte-Anne Hospital’s local ethics committee. Consent for publication The patients signed informed consent forms before treatment began. Conflict of interest statement The authors declare that they have no conflicts of interest directly related to the topic of this article. Funding statement The authors declare that they have not received any funding. Acknowledgements We would like to thank the laboratory technicians at GHU Paris - Psychiatry and Neuroscience, Sainte-Anne Hospital for their assistance. References 1. Capper D, Jones DTW, Sill M, Hovestadt V, Schrimpf D, Sturm D, et al. DNA methylation-based classification of central nervous system tumours. Nature. 22 mars 2018;555(7697):469‑74. https://doi.org/10.1038/nature26000 2. Louis DN, Perry A, Wesseling P, Brat DJ, Cree IA, Figarella-Branger D, et al. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro-Oncol. 2 août 2021;23(8):1231‑51. https://doi.org/10.1093/neuonc/noab106 3. Tauziède-Espariat A, Pierron G, Siegfried A, Guillemot D, Uro-Coste E, Nicaise Y, et al. The EP300:BCOR fusion extends the genetic alteration spectrum defining the new tumoral entity of « CNS tumors with BCOR internal tandem duplication ». Acta Neuropathol Commun. 2 nov 2020;8(1):178. https://doi.org/10.1186/s40478-020-01064-8 4. Wu Z, Rajan S, Chung HJ, Raffeld M, Panneer Selvam P, Schweizer L, et al. Molecular and clinicopathologic characteristics of gliomas with EP300::BCOR fusions. Acta Neuropathol (Berl). déc 2022;144(6):1175‑8. https://doi.org/10.1007/s00401-022-02508-2 5. Tauziède-Espariat A, Pierron G, Guillemot D, Bochaton D, Watson S, Masliah-Planchon J, et al. CNS tumors with YWHAE:NUTM2 and KDM2B-fusions present molecular similarities to extra-CNS tumors having BCOR internal tandem duplication or alternative fusions. Acta Neuropathol Commun. oct 2021;9(1):176. https://doi.org/10.1186/s40478-021-01279-3 6. Sturm D, Orr BA, Toprak UH, Hovestadt V, Jones DTW, Capper D, et al. New Brain Tumor Entities Emerge from Molecular Classification of CNS-PNETs. Cell. févr 2016;164(5):1060‑72. https://doi.org/10.1016/j.cell.2016.01.015 7. Al-Battashi A, Al Hajri Z, Perry A, Al-Kindi H, Al-Ghaithi I. A Cerebellar High-Grade Neuroepithelial Tumour with BCOR Alteration in a five-year-old Child: A case report. Sultan Qaboos Univ Med J. mai 2019;19(2):e153‑6. https://doi.org/10.18295/squmj.2019.19.02.012 8. Appay R, Macagno N, Padovani L, Korshunov A, Kool M, André N, et al. HGNET-BCOR Tumors of the Cerebellum: Clinicopathologic and Molecular Characterization of 3 Cases. Am J Surg Pathol. sept 2017;41(9):1254‑60. https://doi.org/10.1097/PAS.0000000000000866 9. Bouchoucha Y, Tauziède-Espariat A, Gauthier A, Guillemot D, Bochaton D, Vibert J, et al. Intra- and extra-cranial BCOR-ITD tumours are separate entities within the BCOR-rearranged family. J Pathol Clin Res. mai 2022;8(3):217‑32. https://doi.org/10.1002/cjp2.255 10. Ferris SP, Velazquez Vega J, Aboian M, Lee JC, Van Ziffle J, Onodera C, et al. High-grade neuroepithelial tumor with BCOR exon 15 internal tandem duplication-a comprehensive clinical, radiographic, pathologic, and genomic analysis. Brain Pathol Zurich Switz. mai 2019; https://doi.org/10.1111/bpa.12747 11. Kirkman MA, Pickles JC, Fairchild AR, Avery A, Pietsch T, Jacques TS, et al. Early Wound Site Seeding in a Patient with Central Nervous System High-Grade Neuroepithelial Tumor with BCOR Alteration. World Neurosurg. août 2018;116:279‑84. https://doi.org/10.1016/j.wneu.2018.05.158 12. Paret C, Russo A, Otto H, Mayer A, Zahnreich S, Wagner W, et al. Personalized therapy: CNS HGNET-BCOR responsiveness to arsenic trioxide combined with radiotherapy. Oncotarget. déc 2017;8(69):114210‑25. https://doi.org/10.18632/oncotarget.23174 13. Rao S, Mitra S, Sugur H, Vazhayil V, Rao BRM, Annayappa SK, et al. Central nervous system high grade neuroepithelial tumor with BCOR immunopositivity: Is there a molecular heterogeneity? Brain Tumor Pathol. janv 2021;38(1):41‑9. https://doi.org/10.1007/s10014-020-00381-z 14. Wang R, Guan W, Qiao M, Zhang Y, Zhang M, Wang K, et al. CNS tumor with BCOR internal tandem duplication: Clinicopathologic, molecular characteristics and prognosis factors. Pathol Res Pract. août 2022;236:153995. https://doi.org/10.1016/j.prp.2022.153995 15. Yoshida Y, Nobusawa S, Nakata S, Nakada M, Arakawa Y, Mineharu Y, et al. CNS high-grade neuroepithelial tumor with BCOR internal tandem duplication: a comparison with its counterparts in the kidney and soft tissue. Brain Pathol Zurich Switz. Sep 2018;28(5):710‑20. https://doi.org/10.1111/bpa.12585 16. Fukuoka K, Kanemura Y, Shofuda T, Fukushima S, Yamashita S, Narushima D, et al. Significance of molecular classification of ependymomas: C11orf95-RELA fusion-negative supratentorial ependymomas are a heterogeneous group of tumors. Acta Neuropathol Commun. Dec 2018;6(1):134. https://doi.org/10.1186/s40478-018-0630-1 17. Ishi Y, Shimizu A, Takakuwa E, Sugiyama M, Okamoto M, Motegi H, et al. High-grade neuroepithelial tumor with BCL6 corepressor-alteration presenting pathological and radiological calcification: A case report. Pathol Int. mars 2021; https://doi.org/10.1111/pin.13083 18. Vewinger N, Huprich S, Seidmann L, Russo A, Alt F, Bender H, et al. IGF1R Is a Potential New Therapeutic Target for HGNET-BCOR Brain Tumor Patients. Int J Mol Sci. juin 2019;20(12). https://doi.org/10.3390/ijms20123027 19. Wang W, Zhang A, Li Y, Wang D, Chen L, Li Q, et al. Clinical, pathological, and molecular features of central nervous system tumors with BCOR internal tandem duplication. Pathol Res Pract. juill 2024;259:155367. https://doi.org/10.1016/j.prp.2024.155367 20. Bremer J, Kottke R, Johann PD, von Hoff K, Brazzola P, Grotzer MA, et al. A single supratentorial high-grade neuroepithelial tumor with two distinct BCOR mutations, exceptionally long complete remission and survival. Pediatr Blood Cancer.mai 2020; 67(7):e28384. https://doi.org/10.1002/pbc.28384 21. Mardi L, Tauziède-Espariat A, Guillemot D, Pierron G, Gigant P, Mehdi L, et al. Bcor Immunohistochemistry, And Not SATB2, Is A Sensitive And Specific Diagnostic Biomarker For Cns Tumors With BCOR Internal Tandem Duplication. Histopathology. juill 2021; 79(5):891-894. https://doi.org/10.1111/his.14439 22. Ebrahimi A, Waha A, Schittenhelm J, Gohla G, Schuhmann MU, Pietsch T. BCOR::CREBBP fusion in malignant neuroepithelial tumor of CNS expands the spectrum of methylation class CNS tumor with BCOR/BCOR(L1)-fusion. Acta Neuropathol Commun. avr 2024;12(1):60. https://doi.org/10.1186/s40478-024-01780-5 23. Yamazaki A, Arai Y, Fukuoka K, Nakano Y, Hama N, Nakata S, et al. Diffusely infiltrating glioma with CREBBP-BCORL1 fusion showing overexpression of not only BCORL1 but BCOR: A case report. Brain Tumor Pathol. juill 2022;39(3):171‑8. https://doi.org/10.1007/s10014-022-00435-4 24. Vroobel KM, Khalid S, Cavalchini S, Attygalle AD. A Novel EPC1 :: KDM2B Fusion in High-grade Endometrial Stromal Sarcoma. Int J Gynecol Pathol Off J Int Soc Gynecol Pathol. nov 2024;43(6):612‑6. https://doi.org/10.1097/PGP.0000000000001026 25. Kao YC, Sung YS, Zhang L, Chen CL, Huang SC, Antonescu CR. Expanding the Molecular Signature of Ossifying Fibromyxoid Tumors with 2 Novel Gene Fusions: CREBBP-BCORL1 and KDM2A-WWTR1. Genes Chromosomes Cancer. janv 2017;56(1):42‑50. https://doi.org/10.1002/gcc.22400
Copyright: © 2025 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License ( https://creativecommons.org/licenses/by/4.0/ ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver ( https://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated. |