|
|
|
Free Neuropathology 5:23 (2024) |
|
Letter |
|
YAP1 fusion-positive ependymoma presenting in an adult with a pigmented phenotype and association with superficial siderosis |
|
Osorio Lopes Abath Neto1, Leonardo Furtado Freitas2, Martha Quezado3, Zied Abdullaev3, Kenneth Aldape3 |
|
|
Corresponding author: |
|
Submitted: 19 August 2024 |
|
Keywords: Pigmented, Ependymoma, YAP1, Siderosis, DNA methylation |
|
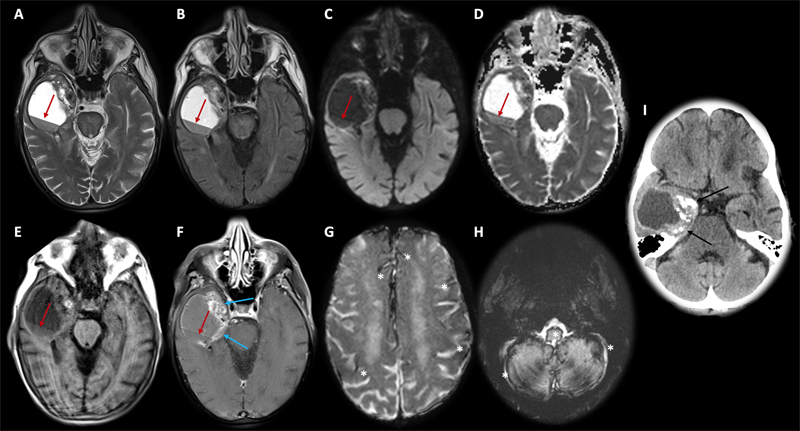
Ependymomas containing pigmented tumor cells are rare, with only 17 reported cases in the literature1,2,3,4, most of which arrising from the fourth ventricle or adjacent locations in the infratentorial compartment. The pigment frequently consists of neuromelanin5, lipofuscin, or a combination of both1. The cases reported so far have not been characterized with molecular testing, except for the index case of Himstead et al.1, which was shown to represent a posterior fossa type B ependymoma by methylation profiling, as expected from the demographics (46-year-old female) and tumor location (floor of the fourth ventricle). Here we describe a case of a pigmented ependymoma with multiple unusual features: adult age, location in the supratentorial compartment, presence of a YAP1 fusion, and association with superficial siderosis. This case expands the spectrum of demographic and morphologic features associated with YAP1 fusion-positive ependymomas and represents to our knowledge the first supratentorial pigmented ependymoma with complete molecular characterization. A 66-year-old female with a history of smoking and localized squamous cell carcinoma of the right nare diagnosed 4 years prior presented to the emergency room with one week of confusion and falls, which had worsened in the last day. Brain imaging revealed a heterogeneously enhancing right anterior temporal lobe mass with solid and cystic components. There was evidence of hemorrhage within the tumor and in the subarachnoid space, as well as supra- and infratentorial superficial siderosis (Figure 1). The patient underwent gross total tumor resection and recovered well after the surgery.
Figure 1. Axial brain MRI (A–H) and CT (I) images. Large right temporal solid and cystic lesion with blood level (red arrows) and heterogeneous contrast enhancement in the medial margin (blue arrows). There was no restricted diffusion (C and D). T2* magnetic susceptibility sequence (G and H) showed extensive supra- and infratentorial superficial siderosis (white asterisks). Multiple punctate calcifications along the solid tumoral medial margin are seen on CT imaging (I, black arrows). The neoplasm was composed of relatively monomorphic cells with round to oval nuclei with a dispersed chromatin distribution and variable amounts of fibrillary cytoplasm. Scattered areas showed perivascular pseudorosettes (Figure 2). There was a sharp interface between the tumor and surrounding reactive brain parenchyma, which exhibited astrogliosis and Rosenthal fibers. Multifocal areas of hemorrhage and hemosiderin-laden macrophages were identified in subependymal and superficial cortical areas. Many tumoral cells contained a coarse dark cytoplasmic pigment, which was not highlighted by Fontana Masson or iron stains, showed autofluorescence and PAS positivity after diastase treatment, and was electron-dense and associated with vacuoles on ultrastructural studies, most consistent with lipofuscin. There were no areas of necrosis and mitotic figures were not apparent. Neoplastic cells were positive for GFAP, negative for synaptophysin, and showed a prominent paranuclear dot-like staining pattern for EMA, but only rare cells showed OLIG2 and SOX10 expression.
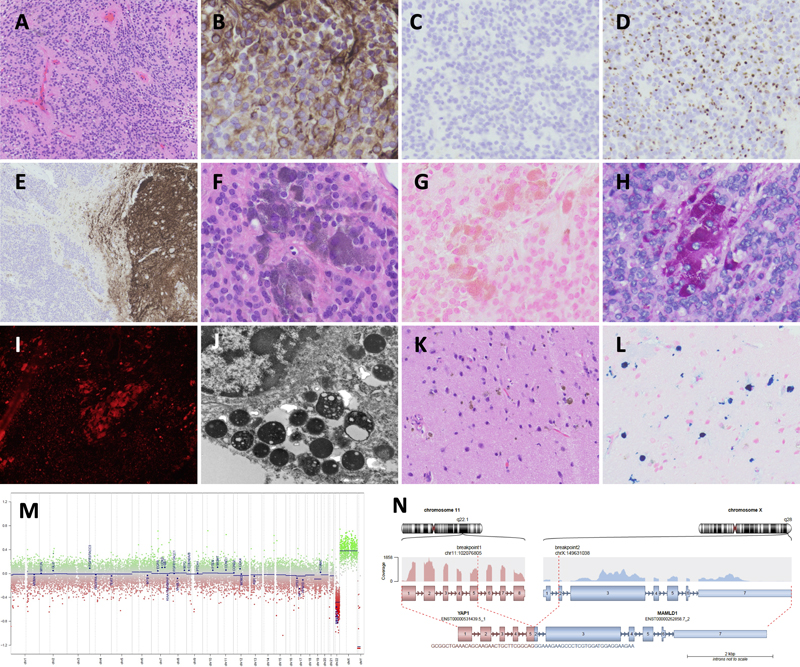
Figure 2. Morphologic and molecular features of the pigmented ependymoma. The neoplasm is composed of monomorphic cells with oval nuclei arranged in an ependymoma-like architecture with vascular pseudorosettes (A; H⁍&⁍E, 100X). Neoplastic cells are positive for GFAP (B; 400X), negative for OLIG2 (C; 200X), and show a prominent paranuclear dot-like staining pattern for EMA (D; 200X). Synaptophysin (E; 100X) is negative in the tumor but positive in the adjacent neuropil at the right. In multiple foci of the tumor, neoplastic cells contain cytoplasmic accumulation of a dark pigment (F; H⁍&⁍E, 400X), which is negative for melanin (G; Fontana Mason, 400X), positive for PAS with diastase (H; 400X) and shows autofluorescence on fluorescence microscopy (I; 100X). Electron microscopy (J; 25000X) shows electron-dense structures associated with vacuoles within the cytoplasm of the tumor cells. Superficial areas of the cortex uninvolved by the tumor contain dispersed deposits of hemosiderin (K; H⁍&⁍E, 200X), which are positive with an iron stain (L; iron, 200X). Molecular testing revealed copy number loss of chromosome 22q (M; copy number variation profile from methylation analysis) and detection of a fusion involving YAP1 and MAMLD1 (N). DNA methylation profiling resulted in concordant matches with high confidence scores to the YAP1 fusion-altered supratentorial ependymoma class in multiple versions of DNA methylation classifiers (DFKZ version 12b6 score 1.0, Bethesda version 2 score 0.96). An RNA exome fusion panel detected a YAP1::MAMLD1 fusion, consistent with the methylation-based classification. Ependymomas with YAP1 fusion in adults are exceedingly rare, with only a few reported cases outside the pediatric population. In a series of 13 confirmed YAP1 fusion-positive ependymomas at the National Cancer Institute (NCI), only two were identified in adults: a 45-year-old female and an 86-year-old female. Both cases occurred in the cerebral hemispheres (unknown specific location for the first case and right occipital lobe on the second), but none had pigmented cells or evidence of prior hemorrhage. This seems to suggest that the presence of pigmented neoplastic cells in ependymomas is unrelated to the underlying molecular abnormalities, with now two confirmed cases having differing molecular classification: supratentorial YAP1 fusion-positive and posterior fossa B ependymoma1. Interestingly, all three of the YAP1 fusion-positive tumors in the adult demographic (this case and the two cases at NCI) were females, in keeping with the predominance of this tumor in females in pediatric series6. This case also showed imaging evidence of superficial siderosis involving the supra- and infratentorial compartments, confirmed in the surgical specimen with the presence of hemosiderin deposition in neocortical sections adjacent to and within a small subependymal area overlying the tumor. Superficial siderosis has been rarely reported in spinal ependymoma cases7,8. Considering the combination of siderosis indicating chronic bleeding and the presence of prominent Rosenthal fibers and calcifications, all morphologic markers of a longstanding reactive process, the tumor we report most likely had a slow growth. Furthermore, the presence of lipofuscin argues in favor of postmitotic tumor cells that have aged long enough to allow for the accumulation of non-degradable proteins within the cytoplasm. Lipofuscin aggregates in neurons are a hallmark of senescence9, and YAP1 fusion-positive ependymomas are likely to arise from neural progenitor cells10. The understanding of the behavior of YAP1 fusion-positive ependymomas is limited given its rarity but in pediatric series they appear to show a favorable prognosis compared to other ependymal neoplasms11. The patient of this case underwent successful gross total resection with uneventful recovery, but long-term follow up data and accumulation of more cases are needed to reliably establish expected outcomes for these tumors. Conflicts of Interest Statement The authors have no conflicts of interest to report. Funding Statement The authors acknowledge that they received no funding in support for this work. References 1. Himstead AS, Perez-Rosendahl M, Fote GM, Zhang A, Kim MG, Floriolli D, et al. Pigmented ependymoma, a tumor with predilection for the middle-aged adult: case report with methylation classification and review of 16 literature cases. Free Neuropathol 2022;8;3:3-16. https://www.doi.org/10.17879/freeneuropathology-2022-4076 2. Malhotra A, Rao S, Santhoshkumar R, Muralidharan N, Mitra S, Shetty S. Pigmented Ependymoma of the Fourth Ventricle-A Curious Entity: Report of a Rare Case With Review of Literature. Int J Surg Pathol 2021;29(1):80-84. https://www.doi.org/10.1177/1066896920926700 3. Chan AC, Ho LC, Yip WW, Cheung FC. Pigmented ependymoma with lipofuscin and neuromelanin production. Arch Pathol Lab Med 2003;127(7):872-5. https://www.doi.org/10.5858/2003-127-872-PEWLAN 4. Rosenblum MK, Erlandson RA, Aleksic SN, Budzilovich GN. Melanotic ependymoma and subependymoma. Am J Surg Pathol 1990;14(8):729-36. https://www.doi.org/10.1097/00000478-199008000-00005 5. McCloskey JJ, Parker JC Jr, Brooks WH, Blacker HM. Melanin as a component of cerebral gliomas: the melanotic cerebral ependymoma. Cancer 1976;37(5):2373-9. https://www.doi.org/10.1002/1097-0142(197605)37:5<2373::aid-cncr2820370529>3.0.co;2-2 6. Pajtler KW, Witt H, Sill M, Jones DT, Hovestadt V, Kratochwil F, et al. Molecular Classification of Ependymal Tumors across All CNS Compartments, Histopathological Grades, and Age Groups. Cancer Cell 2015;11;27(5):728-43. https://www.doi.org/10.1016/j.ccell.2015.04.002 7. Pikis S, Cohen JE, Vargas AA, Gomori JM, Harnof S, Itshayek E. Superficial siderosis of the central nervous system secondary to spinal ependymoma. J Clin Neurosci 2014;21(11):2017-9. https://www.doi.org/10.1016/j.jocn.2014.05.020 8. Zhuang J, Duan Q, Liang C, Chang Y, Yin D. Superficial siderosis of the central nervous system caused by myxopapillary ependymoma of cauda equine: a case report. Neurol Sci 2024;45(3):1303-1306. https://www.doi.org/10.1007/s10072-023-07099-8 9. Moreno-García A, Kun A, Calero O, Medina M, Calero M. An Overview of the Role of Lipofuscin in Age-Related Neurodegeneration. Front Neurosci 2018;5:12:464. https://www.doi.org/10.3389/fnins.2018.00464 10. Eder N, Roncaroli F, Domart MC, Horswell S, Andreiuolo F, Flynn HR, et al. YAP1/TAZ drives ependymoma-like tumour formation in mice. Nat Commm 2020;11(1):2380. https://www.doi.org/10.1038/s41467-020-16167-y 11. Andreiuolo F, Varlet P, Tauziède-Espariat A, Jünger ST, Dörner E, Dreschmann V, et al. Childhood supratentorial ependymomas with YAP1-MAMLD1 fusion: an entity with characteristic clinical, radiological, cytogenetic and histopathological features. Brain Pathol 2019;29(2):205-216. https://www.doi.org/10.1111/bpa.12659
Copyright: © 2024 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |