|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Free Neuropathology 5:24 (2024) |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Original Paper |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Assessment of intraepidermal nerve fiber densities in 5 µm sections from arm and leg – a search for normative age-related values |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Linnéa Ekman1, Lars B. Dahlin1, 2, 3, Elisabet Englund4 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Corresponding author: |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Submitted: 19 August 2024 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Keywords: Intraepidermal nerve fiber density, Skin biopsy, Peripheral neuropathy, Small nerve fiber neuropathy |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Abstract
Background and aims: Normative values are lacking regarding intraepidermal nerve fiber density (IENFD) in thin sections of 5 µm. Thus, we aimed to assess IENFD in thin sections in a healthy adult population as well as to investigate whether IENFD is related to age, sex, and site of excision. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
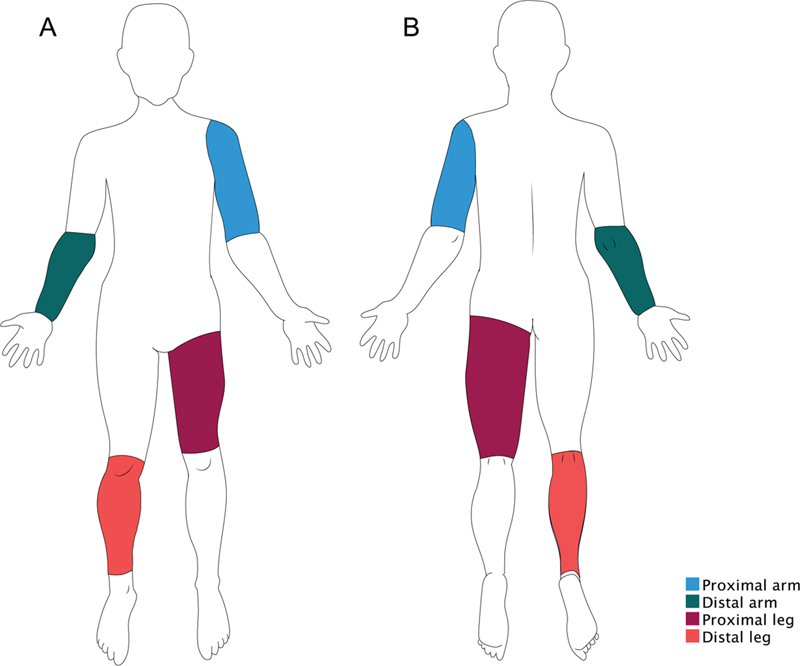
Introduction The use of skin biopsy with subsequent assessment of the intraepidermal nerve fiber density (IENFD) has been developed over the last three decades.1 The assessment can reveal loss of small A and unmyelinated C fibers in the epidermal skin layer. An early study used IENFD to demonstrate small fiber neuropathy (SFN), where no underlying cause was known and nerve conduction was normal.2 Another study reported a high sensitivity (88 %) in diagnosing SFN through IENFD.3 Beyond the area of SFN, studies have highlighted the utility of evaluating IENFD at the distal leg in peripheral neuropathies associated with conditions such as diabetes mellitus,4,5 systemic lupus erythematosus,6 alcohol dependency,7 and hereditary transthyretin amyloidosis polyneuropathy.8 Guidelines on the use of skin biopsy and IENFD for diagnosing peripheral neuropathy were published in 2005, as requested by the European Federation of Neurological Societies.9 The recommended methodology entails obtaining a 3 mm punch skin biopsy at the distal leg, immunostaining with the Protein Gene Product (PGP) 9.5 antibody, and quantification of IENF in at least three 50 µm thick sections through either bright-field or immunofluorescence microscopy. PGP 9.5 is a ubiquitin hydrolase that is highly expressed in neurons and serves as an effective marker for the finest nerves, such as skin innervation, outperforming other markers such as neuron-specific enolase and neurofilament10,11 Two large multi-center studies have established reference values for IENFD in 50 µm sections obtained from the distal leg based on compiled data from healthy individuals, one for each microscopy method.12,13 Both studies found similar age- and sex-related effects on IENFD values, where IENFD declined with age and women have slightly higher densities than men. However, to our knowledge, handling 50 µm sections to perform immunohistochemical staining is not a routine procedure in most clinical pathology laboratories, thereby not applicable in clinical practice, and hence mostly used for research purposes or in commercial laboratories. Modifications of the method have been proposed where e.g. Koskinen et al measured IENF per epidermal area instead of length in 10 µm sections.14 Thereto, Dabby et al. studied the dermal, and not epidermal, autonomic nerve fibers in 5 µm sections.15 A third modification of the method was developed within the Department of Pathology in Lund, Sweden, where IENFD is assessed in the epidermal layer of 5 µm sections.16,17 The method is possible to employ in an ordinary diagnostic laboratory situation since it requires only standard laboratory equipment and techniques.16,18,19 Through our previous studies, we have learned that IENFDs in the distal leg are lower in people with type 2 diabetes compared to healthy controls, but also that a temporal decline can be found in both populations.20 At the wrist level, however, no impairment in IENFDs could be found within either type 1 or type 2 diabetes in comparison to controls, despite signs of neuropathy in biopsies from a nearby nerve, i.e. the posterior interosseous nerve.16 Other findings of that study included significantly higher densities in women compared to men as well as in hairy skin compared to glabrous skin. We have also shown that the nerve fiber assessment in 5 µm sections has a high inter- and intra-rater reliability.18,20 However, reference values are lacking for our modified method, which is a crucial step towards enabling clinical evaluation and distinction between health and illness. The overall aim of this study was to assess IENFD in thin 5 µm skin sections in a healthy population with the attempt to establish normative data for potential future diagnostic use. Additionally, we aimed to explore any variations in IENFD across different ages, sexes, and excision sites, to enhance the understanding of skin innervation throughout the body. Methods and Materials Ethics statement The study was approved by the Swedish Ethical Review Authority as ethical permission no. 2020-03597. The study was conducted in accordance with the Declaration of Helsinki. Study population and skin tissue sampling Samples were manually selected and collected from archival tissue material in the Clinical Department of Pathology in Lund-Malmö, Sweden, between October 2020 and July 2023. All the archival tissue had been previously examined as the primary sampling was based on clinical diagnostic issues, such as nodules or pigmented lesions requiring histopathologic examination, and stored according to the Swedish Biobank Act. The pathology database system was searched for tissue material comprising excisions or diagnostic biopsies obtained in the arm or leg of adult individuals aged 18 years or above in considerable health. Each specimen’s distal ends, around a central abnormality in the ovoid-shaped excision, were checked for morphologically normal appearance and could be included if accepted. Causes for exclusion were inflammation, signs of itching or scratching, hyperplastic epithelium, or scarred tissue. Skin samples from both arm and leg were further divided into two categories: the proximal or the distal part of the limb. The proximal arm was defined as the region extending from the level of the glenohumeral joint to just proximal to the elbow, while the distal arm included the elbow and reached down to the wrist. Correspondingly, the proximal leg referred to the thigh (distal to the inguinal ligament), whereas the distal leg included the knee and continued down to the ankle (Fig. 1). Samples were thus included if the site of excision (or biopsy) was anatomically defined, and the presence of healthy tissue could be confirmed in either the whole or a part of the specimen. Correlating paraffin-embedded tissue blocks were retrieved from the archive to be re-sectioned and immunohistochemically stained.
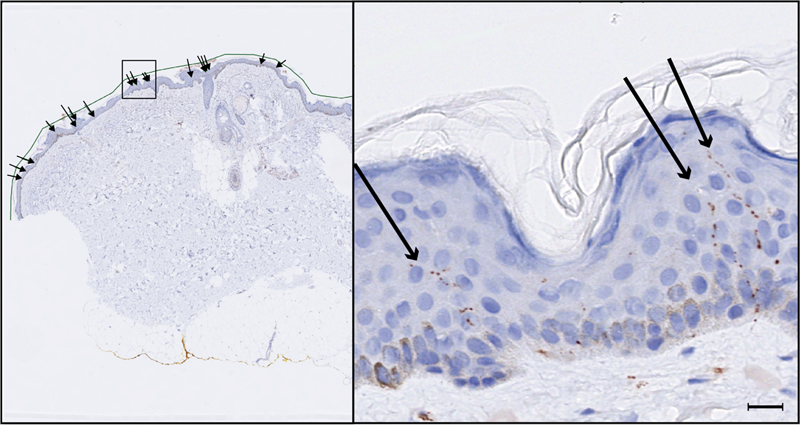
Figure 1. Anatomical classification of skin tissue samples included in the study The web-based medical record system Melior, used in the health care system in Region Skåne, Sweden, was searched for information on prevalent diseases and potential causes, or symptoms, of neuropathy. Exclusion criteria were diabetes mellitus, Lyme disease, Parkinson’s disease, uremia, multiple sclerosis, amyloidosis, scleroderma, dysregulated thyroid function, alcoholism, B12 deficiency, cytostatic treatment, diagnosed neuropathy, or nerve damage affecting the specific limb. Other causes for exclusion from the study were insufficient amount of tissue as well as suboptimal histochemical quality of the sections. Immunohistochemistry All skin biopsies and excisions were uniformly short-time fixed in a 4 % buffered formaldehyde solution following the standard procedures of the clinical diagnostic laboratory. After being in fixation for at least 24 hours, the samples were dehydrated and embedded in paraffin. Upon inclusion in the study, the paraffin-embedded tissue blocks were re-sectioned at 5 µm and mounted on glass for immunohistochemical staining with, generally, two serial sections on each glass. The sections were dried at 60° C for one hour, de-waxed, rehydrated, and microwave-pre-treated in 10 mM citrate buffer (pH 6.0) for 19 minutes at 750 W. The automated immunostainer (TechMate 500 Plus; Dako) was implemented for immunohistochemical staining and the rabbit polyclonal Protein Gene Product (PGP) 9.5 antibody (Cell Marque, Rocklin, USA) was used as the primary antibody, in a 1 : 3000 dilution. All samples were sequentially sectioned and stained batch-wise, using the same procedure, in the laboratories of Lund and Malmö, Sweden. Assessment of IENFD Assessment of IENFD was performed manually in Sectra IDS7, where the scanned tissue sections could be viewed and examined microscopically. The epidermal layer was digitally measured and intraepidermal nerve fibers (IENF) were identified. The number of individual PGP 9.5-positive fibers was counted according to our previously published criteria, however with a new criterion for the minimal length of fibers to be counted, i.e. the fiber was counted if the length measured ≥ 15 µm (Fig. 2).16, 20 Fibers that branched within the epidermal layer were counted as a single fiber. The highest number obtained from any of the serial sections was recorded. To obtain IENFD, the number of nerve fibers was related to the length of the epidermal layer of each sample and expressed as fibers/mm.
Figure 2. Assessment of IENFD in a 5 µm section Statistical analyses The data on IENFD were not normally distributed and thus presented as a median with 25 and 75 percentiles. Data was stratified by age, with the first group comprising individuals aged 18–29 years, followed by groups in 10-year intervals, and the final group including participants aged 80 years and older. The IENFDs were compared between age groups, excision sites, and sex using the Kruskal-Wallis test and Dunn’s post-hoc testing with Bonferroni correction. An additional group comparison was made between young (18–44 years), middle-aged (45–65 years), and older adults (> 65 years). Quantile regression analyses were applied to investigate the effect of age and sex on IENFD across deciles (0.1–0.9) on each of the excision sites. The model was adjusted with a quadratic term for age. P-values < 0.05 were considered statistically significant. Statistical analyses were performed using SPSS Statistics version 27. Results A total of 602 samples were collected from 591 unique subjects, all considered healthy, ranging in age from 18 to 97 years (median 55 years; 295 women and 296 men). Values of IENFD ranged between 0 and 8.6 fibers/mm in the entire cohort. A complete absence of nerve fibers was noted in 34 samples. Median IENFD values at the four excision sites (proximal arm, distal arm, proximal leg, and distal leg as defined in Methods) are presented for men and women as well as for each age group in Table 1.
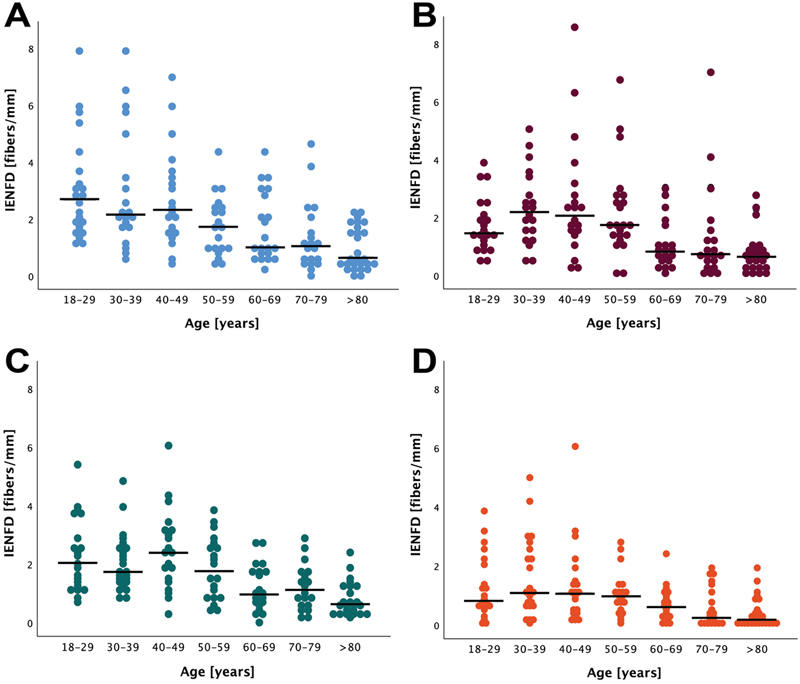
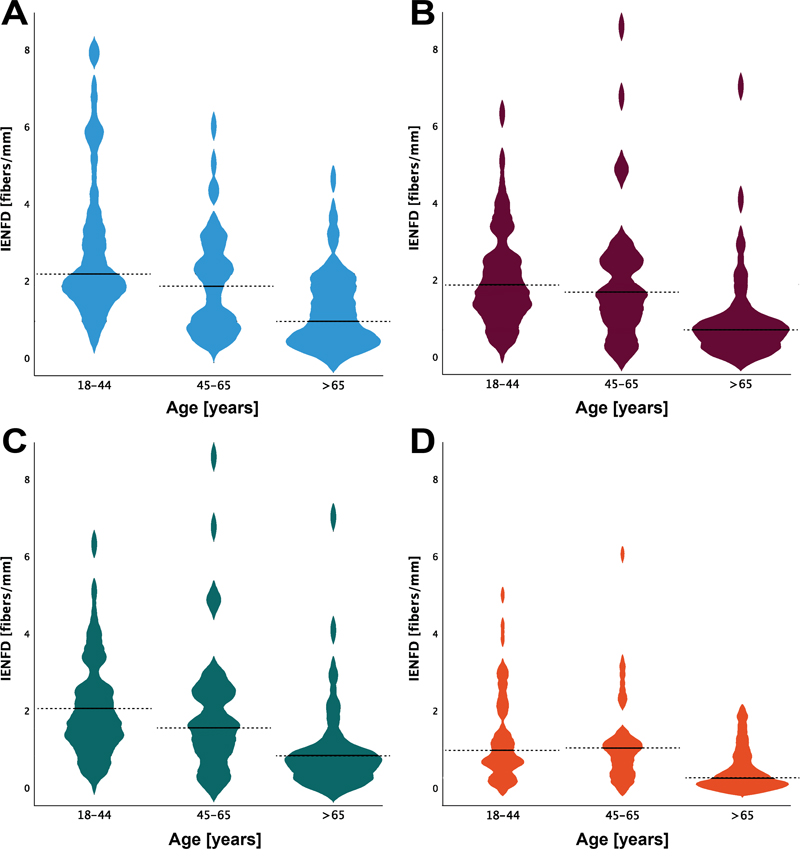
When comparing the four excision sites, overall differences were found among the three lower age groups for men (p < 0.019), and within the groups aged 18–29, 50–59, and > 80 years for women (p < 0.013). Post-hoc testing showed generally higher IENFD in the arm compared to the leg (p < 0.032). Differences between proximal and distal portions of the leg were only found for women aged 50–59 years (p = 0.024). Between the proximal and distal arm, however, no significant differences were observed. Regarding age, statistically significant differences in IENFD were observed when testing across all age groups at all four excision sites for both men and women (p < 0.031; Fig. 3). Post-hoc testing revealed that these differences were primarily between the eldest group (> 80 years) and the four younger groups (18–29, 30–39, 40–49, and 50–59 years), though the pattern was rather inconsistent. When the cohort was divided into three broader age categories – young (18–44 years), middle-aged (45–65 years), and older adults (> 65 years) – the differences became more pronounced (p < 0.005). Post-hoc analyses indicated that IENFDs were lower at all excision sites in both men and women aged > 65 compared to the young group (p < 0.015). The IENFDs were also lower among the older adults in comparison to the middle-aged adults at the proximal (p < 0.029) and distal leg (p < 0.018), as well as at the distal arm (p < 0.045). Notably, no differences in IENFD were found between the young and middle-aged groups (Fig. 4).
Figure 3. Levels of IENFD at four anatomical skin excision sites stratified in age deciles
Figure 4. Levels of IENFD at four anatomical skin excision sites in young, middle-aged, and older adults Age and sex differences were further investigated using quantile regression analysis, which indicated an age impact for the first and second quantiles at the proximal arm (decrease by 0.04 to 0.05 fibers/mm per year, p < 0.021), as well as in the ninth quantile at the proximal leg (increase of 0.25 fibers/mm per year, p = 0.011). Impact of sex was found within quantiles 3 to 6 for the distal arm and quantiles 4 to 6 at the proximal leg, with higher predicted IENFD in women compared to men (0.47–0.68 fibers/mm, p < 0.014). Discussion The primary objective of this present study was to establish normative values for IENFD assessment in thin 5 µm sections, with the additional goal of investigating potential affecting factors in terms of age, sex, and anatomical site of excision. Given our previous findings regarding a temporal decline in IENFD for both people with and without type 2 diabetes mellitus,20 we hypothesized an age-dependency for IENFD where densities decrease with advancing age. This hypothesis was further supported by the previous IENFD reference materials, although assessed in thicker sections of 50 µm.12,13 While we did not identify a clear pattern when comparing IENFD across age deciles, we found significantly lower IENFD levels in individuals aged 65 years and older, compared to the groups of young and middle-aged adults. This could suggest that an age-related nerve decline may not be linear but rather occurs later in life. A non-linear pattern of age impact on nerve conduction velocities has been demonstrated in rat models where levels remained stable until the last third of life, after which an impairment was observed 21. A comparable trend has also been suggested in humans where nerve conduction velocities and amplitudes appear to worsen with increasing age.22 However, the quantile regression analysis performed in our study did not identify any definitive non-linear relationships between IENFD and age. Moreover, the quantile regression implied sex differences corresponding to the ones found in prior studies,12,13,16,23 but again, not in a conclusive pattern. Interestingly, all studies that found sex differences have consistently observed higher densities among women, implicating e.g. hormonal status as a potential explanatory factor. On the other hand, one study reported no sex-related effects, while another revealed that the initially noted higher IENFD in women lost statistical significance when adjusting for confounding variables, including height and weight.24,25 In this study, IENFD was also compared between the proximal and distal excision sites, as well as between arm and leg, to explore potential variations in nerve fiber distribution across the body. This approach extends previous research on thicker sections, which primarily have been focused on the distal leg.12,13,23 Our findings revealed higher IENFDs in the arm compared to the leg. Higher IENFDs were also found at the proximal portion of the leg, as compared to the distal part, though this was only statistically significant for women aged 50–59 years. This observation aligns with the concept of a proximal-distal gradient, as described by McArthur et al., who reported a 60 % higher density at the thigh compared to the distal leg.24 Umapathi et al. referred to this as the IENFD ratio and used it as a measure of the length-dependent dying-back phenomenon observed in axonal neuropathies.25,26 Although skin innervation in the arms has been investigated priorly, we are not aware of any studies that compare e.g. the density between the proximal and distal arm. A study of pain and touch acuity across different body sites showed better two-point discrimination in the distal arm compared to the shoulder region, but an opposite pattern was observed regarding pain sensitivity to heat.27 This suggests that the mechanoreceptor density is higher in the distal parts, whereas the thermal nociceptors and thus epidermal C-fibers are more abundant in the proximal parts. Hence, a similar pattern as in the legs, i.e. a proximal-distal pattern, could be expected, but we did not find a significant difference between the sites in our study. A substantial proportion of the samples included in our study exhibited markedly low densities, some even as low as zero fibers. The data generally demonstrated greater variability in IENFD than anticipated, leading to inconclusive results. A contributing factor may be the specimen’s anatomical locations, which were roughly categorized into either proximal or distal portions of the arm and leg. It is reasonable to assume variability even within each of these categories. For instance, a mildly traumatized lateral side of the calf probably differs from the protected skin just medial to the tibia, and comparing an area near the wrist with one closer to the elbow may potentially also reveal variations. Previous research has also highlighted distinctions between hairy and glabrous skin at the wrist level.16 The hand and foot were deliberately excluded from the study due to highly area-specific densities (e.g. finger pulp compared to palm of hand) and thus the anticipation of even greater variabilities. The innervation of the hand and foot is unevenly distributed in an intricate pattern across the palm and sole, as demonstrated by Corniani and Saal.28 Although a more nuanced categorization for our study would have been ideal, sparse referral texts necessitated adherence to broader areas. It may also be postulated that the challenge lies in the selection of sufficiently healthy material, as the samples were sourced from specimens submitted for skin pathological examination. Despite efforts to ensure peripheral tissue health and a meticulous review of medical records to exclude nerve-affecting disorders, the possibility of inadvertently including individuals with undetected underlying illnesses cannot be entirely ruled out. The proximity and potential impact of pathology should also be considered, as the skin sections used in the present study were all harvested from tissue blocks comprising excisions of skin lesions. The impact of skin lesions on fiber density might be different depending on the type. For example, in a study by Bröcker et al., the number of nerve fibers was shown to be higher within melanocytic nevi compared to the surrounding tissue, whereas no differences could be observed within cutaneous melanoma metastases.29 Additionally, nerve fiber counts were found to be influenced by tumor properties, such as increasing tumor thickness in cutaneous melanomas leading to decreasing nerve counts.In our study, we focused on obtaining samples from the macroscopically intact outer ends of excisions, where the radicality of the excision could be ensured. In cases where such end snippets were not available, IENFD assessment was only performed if the skin section was sufficiently long to provide a substantial distance from the skin lesion, and the surrounding skin appeared normal and healthy. These precautions were taken to minimize the potential influence of the lesion on nerve fiber density and ensure that the assessment was conducted on skin resembling normal skin. After analysis of a substantial number of sections in this study, it became evident that nerve fibers were being excluded under the preexisting criteria of our method. Consequently, we explored and implemented a modification: counting fibers ≥ 15 µm in length to capture a higher number of solid fibers, while still excluding debris. This modification, differing from our previous studies, proved to be more inclusive. Despite our efforts to adapt the method for thinner sections, we still obtained very low counts in some sections, posing potential challenges in clinical applications where distinguishing between healthy and pathological samples is crucial. Traditional approaches, presenting the 5 percentile as a cut-off threshold for normative values, are deemed impractical for our methodology as this percentile reaches an IENFD of zero fibers/mm for some locations and age spans.12,23,24 In this study, absolute cut-offs could not be established. A recently published article by Aspegren and Pourhamidi has demonstrated promising results using a new method, called estimated IENFD (eIENFD) assessment, in thin sections, produced comparable numbers to the 50-micrometer method.30 This approach utilizes the same thin sectioning and immunohistochemical procedure as in our study. However, the eIENFD method involves counting even smaller fragments than in our proposed method, which may present additional challenges. Despite these challenges, as well as those identified in our study, it is essential to develop a method that is applicable within standard laboratory settings for diagnostic suitability, particularly in Sweden. Therefore, further development of IENFD assessment in thin sections is necessary. During the work, we have also acknowledged some qualitative differences within the samples, emphasizing a shift towards exploring this aspect more comprehensively in forthcoming studies. We are motivated to delve further into this area, as the assessment of IENFD offers an objective investigation of nerve fibers directly related to the region where symptoms manifest. Limitations As previously mentioned, the variable anatomical excision sites are this study’s most important limitation. Standardized sampling on well-described anatomical sites might have yielded a clearer result. Incomplete access to participants’ full medical records poses another limitation. The system Melior encompasses data from all public specialist health care in Region Skåne, yet information about patients residing elsewhere or receiving treatment solely from general practitioners was not available. Conclusion This study provides IENFD values obtained in thin 5 µm sections from both the proximal and distal parts of the arm and leg in a healthy adult population, in a search for potentially normative IENFD values. Differences in IENFD levels were observed across excision sites and age groups, showing notably lower levels among the older groups. However, the data exhibited a greater variability than expected, preventing the identification of clear influencing factors or cut-off values. Further research and continued method development are warranted. Acknowledgments We extend our gratitude to our colleagues at the pathology laboratories in Lund and Malmö for their invaluable assistance in sectioning and staining of all the specimens, and to the dermatopathologists for being patient and helpful. Funding Statement The work was supported by grants from the Swedish Research Council (2021-01942), Skåne University Hospital (2022-974), ALF (2022-projekt0129), the Swedish Diabetes Foundation (DIA2020-492), Elly Olsson’s Foundation for Scientific Research, and the Hans-Gabriel and Alice Trolle-Wachtmeister Foundation for Medical Research. Conflicts of Interest Statement The authors declare no conflict of interest. References 1. Lauria G, Faber CG, Cornblath DR. Skin biopsy and small fibre neuropathies: facts and thoughts 30 years later. J Neurol Neurosurg Psychiatry. 2022;93(9):915-8. https://doi.org/10.1136/jnnp-2021-327742 2. Holland NR, Crawford TO, Hauer P, Cornblath DR, Griffin JW, McArthur JC. Small-fiber sensory neuropathies: clinical course and neuropathology of idiopathic cases. Ann Neurol. 1998;44(1):47-59. https://doi.org/10.1002/ana.410440111 3. Herrmann DN, Griffin JW, Hauer P, Cornblath DR, McArthur JC. Epidermal nerve fiber density and sural nerve morphometry in peripheral neuropathies. Neurology. 1999;53(8):1634-40. https://doi.org/10.1212/wnl.53.8.1634 4. Divisova S, Vlckova E, Srotova I, Kincova S, Skorna M, Dusek L, et al. Intraepidermal nerve-fibre density as a biomarker of the course of neuropathy in patients with Type 2 diabetes mellitus. Diabet Med. 2016;33(5):650-4. https://doi.org/10.1111/dme.12890 5. Narayanaswamy H, Facer P, Misra VP, Timmers M, Byttebier G, Meert T, Anand P. A longitudinal study of sensory biomarkers of progression in patients with diabetic peripheral neuropathy using skin biopsies. J Clin Neurosci. 2012;19(11):1490-6. https://doi.org/10.1016/j.jocn.2011.12.026 6. Omdal R, Mellgren SI, Gøransson L, Skjesol A, Lindal S, Koldingsnes W, Husby G. Small nerve fiber involvement in systemic lupus erythematosus: a controlled study. Arthritis Rheum. 2002;46(5):1228-32. https://doi.org/10.1002/art.10303 7. Kokotis P, Papantoniou M, Schmelz M, Buntziouka C, Tzavellas E, Paparrigopoulos T. Pure small fiber neuropathy in alcohol dependency detected by skin biopsy. Alcohol. 2023;111:67-73. https://doi.org/10.1016/j.alcohol.2023.05.006 8. Leonardi L, Costanzo R, Forcina F, Morino S, Antonini G, Salvetti M, et al. Quantitative sensory testing and skin biopsy findings in late-onset ATTRv presymptomatic carriers: Relationships with predicted time of disease onset (PADO). J Peripher Nerv Syst. 2023;28(3):390-7. https://doi.org/10.1111/jns.12586 9. Lauria G, Cornblath DR, Johansson O, McArthur JC, Mellgren SI, Nolano M, et al. EFNS guidelines on the use of skin biopsy in the diagnosis of peripheral neuropathy. Eur J Neurol. 2005;12(10):747-58. https://doi.org/10.1111/j.1468-1331.2005.01260.x 10. Dalsgaard CJ, Rydh M, Haegerstrand A. Cutaneous innervation in man visualized with protein gene product 9.5 (PGP 9.5) antibodies. Histochemistry. 1989;92(5):385-90. https://doi.org/10.1007/bf00492495 11. Wang L, Hilliges M, Jernberg T, Wiegleb-Edström D, Johansson O. Protein gene product 9.5-immunoreactive nerve fibres and cells in human skin. Cell Tissue Res. 1990;261(1):25-33. https://doi.org/10.1007/bf00329435 12. Lauria G, Bakkers M, Schmitz C, Lombardi R, Penza P, Devigili G, et al. Intraepidermal nerve fiber density at the distal leg: a worldwide normative reference study. J Peripher Nerv Syst. 2010;15(3):202-7. https://doi.org/10.1111/j.1529-8027.2010.00271.x 13. Provitera V, Gibbons CH, Wendelschafer-Crabb G, Donadio V, Vitale DF, Stancanelli A, et al. A multi-center, multinational age- and gender-adjusted normative dataset for immunofluorescent intraepidermal nerve fiber density at the distal leg. Eur J Neurol. 2016;23(2):333-8. https://doi.org/10.1111/ene.12842 14. Koskinen M, Hietaharju A, Kyläniemi M, Peltola J, Rantala I, Udd B, Haapasalo H. A quantitative method for the assessment of intraepidermal nerve fibers in small-fiber neuropathy. J Neurol. 2005;252(7):789-94. https://doi.org/10.1007/s00415-005-0743-x 15. Dabby R, Vaknine H, Gilad R, Djaldetti R, Sadeh M. Evaluation of cutaneous autonomic innervation in idiopathic sensory small-fiber neuropathy. J Peripher Nerv Syst. 2007;12(2):98-101. https://doi.org/10.1111/j.1529-8027.2007.00128.x 16. Thomsen NO, Englund E, Thrainsdottir S, Rosén I, Dahlin LB. Intraepidermal nerve fibre density at wrist level in diabetic and non-diabetic patients. Diabet Med. 2009;26(11):1120-6. https://doi.org/10.1111/j.1464-5491.2009.02823.x 17. Thrainsdottir S. Peripheral polyneuropathy in type 2 diabetes mellitus and impaired glucose tolerance. Correlation between morphology, neurophysiology, and clinical findings. Sweden: Lund University 2009. 18. Ekman L, Thrainsdottir S, Englund E, Thomsen N, Rosén I, Hazer Rosberg DB, et al. Evaluation of small nerve fiber dysfunction in type 2 diabetes. Acta Neurol Scand. 2020;141(1):38-46. https://doi.org/10.1111/ane.13171 19. Pourhamidi K, Dahlin LB, Englund E, Rolandsson O. No difference in small or large nerve fiber function between individuals with normal glucose tolerance and impaired glucose tolerance. Diabetes Care. 2013;36(4):962-4. https://doi.org/10.2337/dc12-1331 20. Ekman L, Pourhamidi K, Englund E, Lagali N, Rolandsson O, Dahlin LB. Temporal trend of small nerve fibre degeneration in people with and without type 2 diabetes mellitus. Diabet Med. 2022;39(3):e14691. https://doi.org/10.1111/dme.14691 21. Verdú E, Butí M, Navarro X. Functional changes of the peripheral nervous system with aging in the mouse. Neurobiol Aging. 1996;17(1):73-7. https://doi.org/10.1016/0197-4580(95)02010-1 22. Taylor PK. Non-linear effects of age on nerve conduction in adults. J Neurol Sci. 1984;66(2-3):223-34. https://doi.org/10.1016/0022-510x(84)90011-x 23. Bakkers M, Merkies IS, Lauria G, Devigili G, Penza P, Lombardi R, et al. Intraepidermal nerve fiber density and its application in sarcoidosis. Neurology. 2009;73(14):1142-8. https://doi.org/10.1212/WNL.0b013e3181bacf05 24. McArthur JC, Stocks EA, Hauer P, Cornblath DR, Griffin JW. Epidermal nerve fiber density: normative reference range and diagnostic efficiency. Arch Neurol. 1998;55(12):1513-20. https://doi.org/10.1001/archneur.55.12.1513 25. Umapathi T, Tan WL, Tan NC, Chan YH. Determinants of epidermal nerve fiber density in normal individuals. Muscle Nerve. 2006;33(6):742-6. https://doi.org/10.1002/mus.20528 26. Umapathi T, Tan WL, Loke SC, Soon PC, Tavintharan S, Chan YH. Intraepidermal nerve fiber density as a marker of early diabetic neuropathy. Muscle Nerve. 2007;35(5):591-8. https://doi.org/10.1002/mus.20732 27. Mancini F, Bauleo A, Cole J, Lui F, Porro CA, Haggard P, Iannetti GD. Whole-body mapping of spatial acuity for pain and touch. Ann Neurol. 2014;75(6):917-24. https://doi.org/10.1002/ana.24179 28. Corniani G, Saal HP. Tactile innervation densities across the whole body. J Neurophysiol. 2020;124(4):1229-40. https://doi.org/10.1152/jn.00313.2020 29. Bröcker EB, Magiera H, Herlyn M. Nerve growth and expression of receptors for nerve growth factor in tumors of melanocyte origin. J Invest Dermatol. 1991;96(5):662-5. https://doi.org/10.1111/1523-1747.ep12470585 30. Aspegren O, Pourhamidi K. Reliable Method for Estimating Nerve Fiber Density in Epidermis Using Routine Histopathologic Tissue Preparation: A Promising Diagnostic Tool for Small Fiber Neuropathy. Appl Immunohistochem Mol Morphol. 2024;32(5):215-21. https://doi.org/10.1097/pai.0000000000001193
Copyright: © 2024 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||