|
|
|||||||||||||||||||||||||||||||||||||
|
Free Neuropathology 4:4 (2023) |
|||||||||||||||||||||||||||||||||||||
|
Review |
|||||||||||||||||||||||||||||||||||||
|
Neurooncology: 2023 update |
|||||||||||||||||||||||||||||||||||||
|
Michel Mittelbronn1-6 |
|||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||
|
Corresponding author: |
|||||||||||||||||||||||||||||||||||||
|
Submitted: 12 February 2023 |
|||||||||||||||||||||||||||||||||||||
|
Keywords: Neuro-oncology, Neuropathology, Brain tumors, Glioblastoma, Brain metastasis, Meningioma |
|||||||||||||||||||||||||||||||||||||
|
Abstract This article presents some of the author’s neuropathological highlights in the field on neuro-oncology research encountered in 2022. Major advances were made in the development of more precise, faster, easier, less invasive and unbiased diagnostic tools ranging from immunohistochemical prediction of 1p/19q loss in diffuse glioma, methylation analyses in CSF samples, molecular profiling for CNS lymphoma, proteomic analyses of recurrent glioblastoma, integrated molecular diagnostics for better stratification in meningioma, intraoperative profiling making use of Raman effect or methylation analysis, to finally, the assessment of histological slides by means of machine learning for the prediction of molecular tumor features. In addition, as the discovery of a new tumor entity may also be a highlight for the neuropathology community, the newly described high-grade glioma with pleomorphic and pseudopapillary features (HPAP) has been selected for this article. Regarding new innovative treatment approaches, a drug screening platform for brain metastasis is presented. Although diagnostic speed and precision is steadily increasing, clinical prognosis for patients with malignant tumors affecting the nervous system remains largely unchanged over the last decade, therefore future neuro-oncological research focus should be put on how the amazing developments presented in this article can be more sustainably applied to positively impact patient prognosis. |
|||||||||||||||||||||||||||||||||||||
|
Introduction For this top ten series regarding the neuro-oncological highlights of the year 2022, the author aimed at selecting pioneering work with a direct link to neuropathology. Apart from previously read papers, the author was inspired by discussions with colleagues and finally screened hundreds of articles limited to the year 2022 in PubMed. In addition, the author “googled” by using the key words “neurooncology” or “neuropathology” in combination with different tumor entity names or laboratory techniques, as it has been shown that for some questions in the biomedical field, Google Scholar search may help to retrieve up to twice more relevant articles than a classic PubMed search or information that is otherwise almost unretrievable [1, 2]. Apart from a high number of pure clinical or neuroradiological papers or case reports that did not directly touch the field of neuropathology and were therefore excluded from this highlight list, the year 2022 can (maybe once again) be summarized under the motto “profiling, profiling, profiling” frequently in combination with machine learning approaches to increase diagnostic velocity and precision. On the other hand, research work with promising treatment approaches making use of the new molecular data was relatively poor being in line with an almost unchanged prognosis for the majority of patients with malignant brain tumors. Certainly, more time is needed to decipher precisely which of these multitudes of new potential therapeutic targets, that nowadays can be detected almost in real-time, will make it into future clinical application. For single topics, the author co-selected two studies due to their similarity or complementarity. The author’s “charts of 2022” in neurooncology reads as follows (not meant in a hierarchical manner but rather in a progression from neuropathological core work to early clinical application):
The author invites you on a joint journey across some of the most recent neurooncological developments touching the field of neuropathology. Of course, this selection is highly subjective, however, the author aimed at selecting very diverse studies from different neurooncological subfields so that the majority of the readership of Free Neuropathology may at least partly be able to share the author’s enthusiasm about the presented studies. 1. New brain tumor entity: high-grade glioma with pleomorphic and pseudopapillary features (HPAP) [3] Even after the neuropathological community has molecularly profiled a huge amount of brain tumor cases worldwide, while also mainly using the same brain tumor methylation classifier, we still struggle from time to time with providing precise diagnoses for particular cerebral tumors. Pratt et al. made use of the brain tumor methylation classifier [https://www.molecularneuropathology.org/mnp based on 15] combined with a next generation sequencing approach using both an amplicon-based brain tumor specific panel [16], as well as the commercial TruSight Oncology 500 panel (TSO 500, Illumina, San Diego, USA) [3]. With this approach, the authors were able to classify 31 previously non-classifiable brain tumors (median patient age was 46.5 years), mainly but not exclusively localized in cortical areas, with highly diverse morphological features, including those of pleomorphic xanthoastrocytoma (PXA), astroblastoma, ependymoma, polymorphous neuroepithelial tumor of the young (PLNTY), as well as IDH wildtype glioblastoma. One important morphological feature was the mainly non-infiltrative growth pattern observed in HPAP. In the brain methylation classifier, these brain tumors did not cluster with any of the known methylation classes in v11.4, however were closest to PXA, MN1-altered astroblastoma and PLNTY. Apart from several frequently encountered mutations in these brain tumors, such as TP53, RB1, NF1 or less frequently NF2 or BRAF-V600E expression, a frequent chromosomal aneuploidy was observed, with a very high rate of a monosomy 13, detected in 28 of 31 cases analyzed. Of note, MGMT promoter methylation was only detected in 1 patient, and a CDKN2A/B deletion in 2 patients of this cohort. As a working entity name, the authors suggested “high-grade glioma with pleomorphic and pseudopapillary features (HPAP)”. The authors proposed 2 molecular subtypes (A and B) without any specific associated genetic or morphological features being associated with those subclasses, however significantly older patients in subtype A as compared to B. Although some of the histologically described morphological features rather indicated a high-grade glioma, the overall survival was not significantly different from pilocytic astrocytoma, PXA and high-grade astrocytoma with piloid features, however, was significantly better than the group of IDH wildtype glioblastomas, therefore, molecularly suggesting a biologically less malignant tumor entity. As the histological picture is highly variable and patient survival not impaired by morphological features of atypia or anaplasia, the authors did not provide definite diagnostic criteria, however, recommended to base diagnosis on the following features: a) no match with a known brain tumor methylation class in the v11.4 (or more recently also v12.5) classifier, b) monosomy of chromosome 13 and c) lack of CDKN2A/B loss. Given the mutational constellation (e.g. BRAF or RB1 mutations), some of the HPAP patients might be eligible for targeted treatment approaches (for comprehensive summary of the HPAP characteristics, please see Table 1). Table 1: Histopathological and molecular features of high-grade glioma with pleomorphic and pseudopapillary features (HPAP)
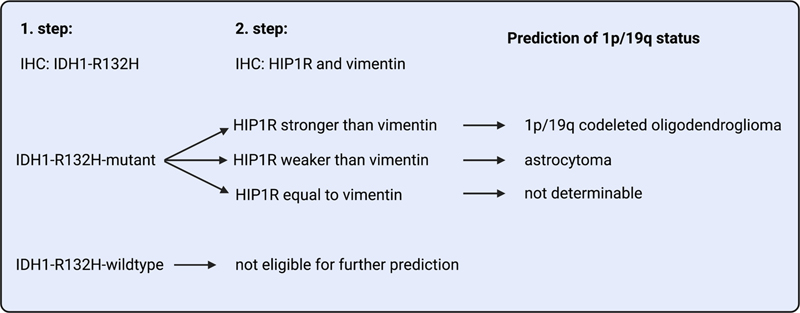
*v11.4 was indicated by the authors, however, also the most recent brain tumor methylation classifier version v12.5 does not yet recognize this tumor entity. 2. Prediction of 1p/19q status by immunohistochemistry in IDH-mutant glioma [4] Nowadays, comprehensive molecular profiling is equal or (for some tumor types) ever superior to histopathology, the previous gold standard. However, broader molecular testing is far from being available in all health care systems across the world. Therefore, it is not only important to promote cutting-edge technology, but also to come up with simple, fast and cheap analytic tools that can be applied in all types of socio-economic systems. Felix et al. started with a mass spectrometric approach to evaluate the most differentially expressed proteins in a series of more than 100 frozen and formalin-fixed, paraffin-embedded diffuse glioma samples with known IDH and 1p/19q status [4]. Out of a larger set of differentially regulated candidate proteins that could have been used as targets for subsequent immunohistochemical (IHC) analyses, the authors selected the ones for which best staining results were obtained, namely vimentin for non-1p/19q-codeleted astrocytomas and HIP1R (huntingtin interacting protein 1 related) for 1p/19q-codeleted oligodendrogliomas. With this simple immunohistochemistry-based approach, the authors were able to predict 1p/19q status in diffuse gliomas with high accuracy (Figure 1). This approach could therefore also be applied in laboratories without state-of-the art molecular pathological pipelines or in less developed countries without broad accessibility to modern molecular testing methods.
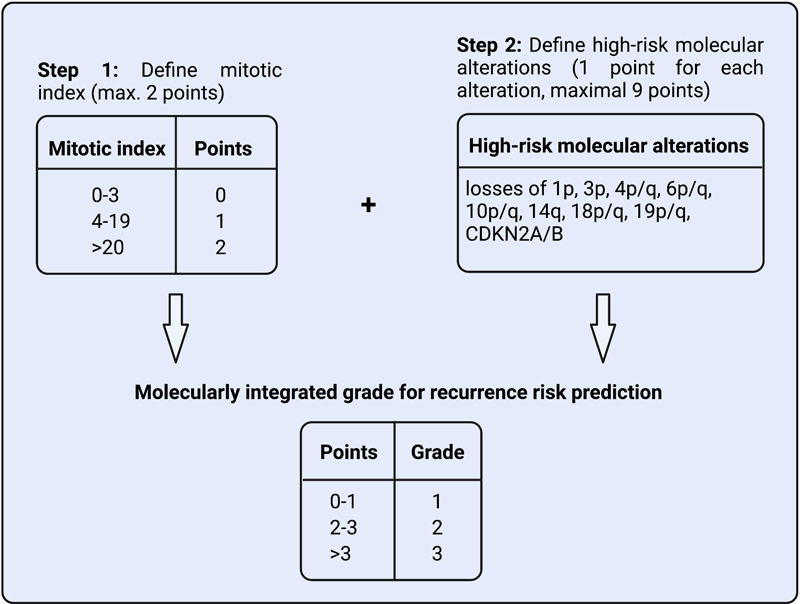
Figure 1: Algorithm for a 2-step immunohistochemical prediction of the 1p/19q status in IDH-mutant gliomas (positivity of tumor cells is evaluated). For each staining, four different expression levels were defined. HIP1R staining was considered positive if expression was observed in the cytoplasm or at the cell membrane. Scores H0 to H3 were defined as follows: H0: less than 10% of tumor cells are weakly positive; H1: 10%-75% of tumor cells are positive, however, less than 30% are strongly positive; H2: more than 50% of the tumor cells are positive, and more than 30% are strongly positive, however, still showing unstained spaces between the tumor cells. The score H2 is also given if the tumor was only moderately positive, however, approximately 100% of the cells showed moderate immunoreactivity in a densely packed manner; H3: approximately 100% of the tumor cells are strongly positive in a diffuse and densely packed manner, with only blood vessels being spared. For the assessment of vimentin (scores V0 to V3 were given), staining of blood vessels was excluded, however, no distinction could be made between reactive and neoplastic glial cells. V0: less than 10% of tumor cells are positive (however, blood vessels and reactive astrocytes could be positive); V1: 10%-20% of tumor cells or tumor cell processes are positive; V2: 20%-70% of the tumor cells with many tumor cell processes are positively labeled, however still 30% or more of the tumor cells are negative; V3: more than 70% of the tumor cells are strongly positive, thereby the tumors exhibit a strong diffuse staining pattern. After this individual assessment, the comparison between HIP1R and vimentin staining was done as shown in Figure 1. 3. Prediction of molecular tumor features from histology by machine learning [5] While molecular analyses in neuropathology are rapidly progressing with regard to speed of analysis and precision of unbiased diagnosis, being always up to a perfect state-of-the-art level cannot currently be guaranteed worldwide. Therefore, machine-learning-based analyses requiring a good microscopic detection system together with powerful computers could be an alternative if prediction would be highly precise. The search for good prediction of molecular properties of tumors from histological images is currently a rapidly progressing research field. Liechty et al. aimed for predicting IDH mutation from histological slides [5]. The authors compared the prediction of a machine learning (ML) system with the prediction of expert neuropathologists’ examination, however, also analyzed if a synergistic approach of ML together with the neuropathological assessment could further enhance the predictive power. For this purpose, they used 801 IDH mutant and wildtype gliomas from the TCGA database, which were split into a training and a validation set (TCGA Research Network: https://www.cancer.gov/tcga). Afterwards, an institutional cohort of 174 IDH mutant and wildtype gliomas was assessed. The neuropathologists were allowed to provide a semiquantitative score between 0 and 1 (with 0.5 for lowest certainty of tumor being either IDH mutant or wildtype), while convolutional neural network (CNN) analyses were applied in ML assessments. No ML approach performed better than the neuropathologists in this task, however, reached similarly good results. Creating an average score of the assessment of two neuropathologists was superior than the prediction of each individual neuropathologist alone. The combination of the prediction of one neuropathologist together with the ML assessment further increased correct prediction as compared to ML or a neuropathologist alone. Of note, the hybrid model of ML and one neuropathologist was similarly precise as compared to the combined score derived from two neuropathologists. Within this relatively restricted cohort of gliomas, ML approaches were able to perform similarly well as trained neuropathologists. Taking into account that the training of a neuropathologist takes several years while ML-based analyses only took a very short time to train; these findings reflect the high potential of ML approaches in diagnostic pathology including neuropathology. This is all the more promising as initial ML training and validation has been performed on an external image set in which potential differences with regard to histology, for example in slide thickness or staining intensities, could have led to improper recognition of histomorphological features. Therefore, computer-assisted diagnostic procedures could be a way to improve diagnostic precision, especially for smaller hospitals or pathological institutes where review by two neuropathologists may not be feasible. One should still consider the current result with caution, however, as still both ML and neuropathologists mixed up IDH wildtype and mutant glioma to a similar extent, clearly indicating limits of predicting molecular features by means of histological analyses only. This task may even be more challenging in small round blue cell tumors or sarcomas, tumor types in which morphological features often correlate even less with the final integrated molecular diagnoses. 4. Histomolecular grading for meningioma [6] Besides the classic grading of brain tumors according to the WHO classification of central nervous system (CNS) tumors, several multicentric studies aimed to more precisely stratify brain tumor patients with regard to their risk of recurrence. In a previous study, it was shown that combining histomorphological assessment of meningioma with methylation analyses led to inverted recurrence risk in some cases, namely that some meningiomas classified as WHO grade I (now CNS WHO grade 1) displayed a higher recurrence risk when applying the meningioma methylation classifier, as compared to cases initially diagnosed as WHO grade 2 tumors according to histomorphological criteria [17]. Along this line, Driver et al. aimed at providing a model for more precise prediction of the clinical behavior of meningiomas going beyond the classic histological grading system [6]. This paper has already been briefly presented in the “Neurooncology: 2022 update” series, however, given the importance of the study and the urgent need for an alignment between different grading schemes, the author of this year’s edition would like to stress the study in more detail again [18]. The authors analyzed a large variety of clinical (gross total or subtotal resection assessed by MRI analyses, progression-free survival), histomorphological (including WHO grade, features of atypia, proliferation and mitotic index) and molecular features (copy number variation, as well as partially targeted mutational profiling and methylation analyses). By correlating all those features with progression-free survival of meningioma patients, the authors finally proposed a new 3-tiered grading scheme taking into account the mitotic count, loss of distinct chromosomal arms or entire chromosomes, or loss of CDKN2A/B. A maximum of 11 points could be obtained (9 for high-molecular risk alterations and 2 for mitotic count), leading to a) grade 1 for 0-1 point, b) grade 2 for 2-3 points and c) grade 3 if 4 or more points were obtained (Figure 2). With this approach, more than 30% of tumors were reclassified as compared to the previously applied WHO grade. Of note, in meningiomas with an integrated tumor score of 3, recurrences could not even be significantly delayed by a gross total resection, which is otherwise a positive factor for longer progression free survival intervals. To avoid confusion between different institutional grading schemes in the future [see also a competing approach here: 19], the WHO should bring different multicenter study groups together and refine the current grading schemes, as the high discrepancies between histomorphological assessment and different integrated scores with regard to patient prognosis has the potential to have a considerably negative impact on patient care. This seems to be all the more important as – in contrast to other chapters in the current WHO classification – the meningioma chapter is still relatively defensive with regard to molecular markers impacting patient prognosis.
Figure 2: Algorithm for integrated grading for recurrence risk prediction in meningioma (mitotic index defined as mitoses per 10 high-power fields). 5. Molecular profiling of CNS lymphoma [7] Primary diffuse large B-cell lymphomas of the CNS (CNS-DLBCL) are the most frequent primary CNS tumors of haematolymphoid origin sharing multiple morphological and molecular features with both its systemic non-CNS and/or secondary CNS counterparts [20]. As the origin of CNS-DLBCL is still not entirely clear and also some of the very recent, promising molecular tools such as DNA methylation-based analyses could not fully distinguish CNS-DLBCL from its non-CNS counterpart, a deeper understanding of the molecular pedigree of CNS-DLBCL is urgently needed. Radke et al. attended to this challenge by studying 51 CNS-DLBCL using transcriptomic and whole genomic analyses and comparing this data set to one derived from 75 lymphomas originating from outside the CNS, the latter including both follicular and DLBC lymphomas [7]. The study could confirm MYD88 (L265P) and CD79B mutations, as well as frequently biallelic CDKN2A loss as very early tumor drivers in CNS-DLBCL. Other frequently encountered alterations comprised activating mutations of BCR signaling and structural variants of IGH, IGL and IGK as well as losses of chromosome 6p. Notably the alteration of chromosome 6p where the human leukocyte antigen (HLA) complex is located may lead to an immune escape from cytotoxic T cells due to limited neoantigen presentation [21]. In addition to their findings on DNA level, Radke et al. could also provide a robust transcriptional signature obtained by RNA sequencing that was able to distinguish CNS-DLBCL from its non-CNS counterparts. They detected higher RNA expression levels of loci associated with aberrant somatic hypermutation phenotypes, although it still remains to be determined what is chicken and what is egg in this association. The CNS-DLBCL group also displayed a higher TERT expression as compared to the group of non-CNS lymphomas, however, without being associated with increased telomere content. Of note, EBV-positive CNS-DLBCL did not share many of the classic mutational hotspots apart from IGH and HLA-DRB locus. It remains to be determined how this important data can be transferred into the daily diagnostic routine for a fast and precise differentiation between a primary CNS-DLBCL, a secondary DLBCL of the CNS, or primary non-CNS DLBCL. This would be all the more important as depending on the method – if immunohistochemical phenotyping or gene expressing profiling is applied – CNS-DLBCL may either be classified as of non-germinal center B-cell like (non-GCB) or late germinal-center exit B-cell origin. Table 2: Molecular differences between CNS diffuse large B-cell lymphoma (DLBCL) and its non-CNS counterpart.
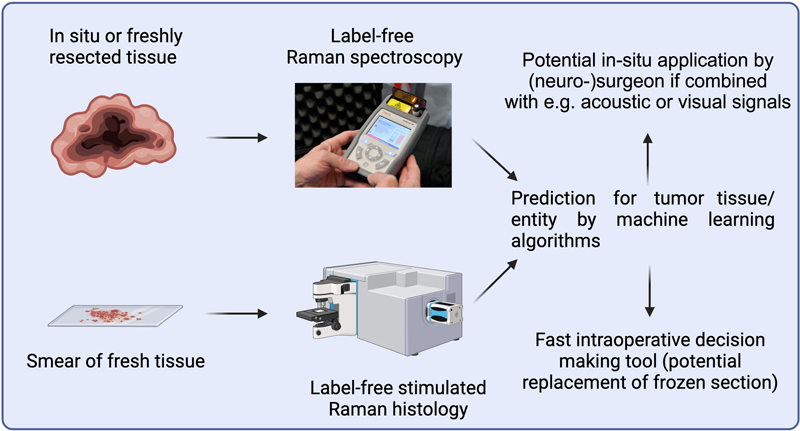
6. Proteomic landscape of primary and recurrent glioblastoma [8] While many current brain tumor studies analyze molecular changes at genomic, epigenomic or transcriptomic levels, large-scale proteomic approaches are largely underrepresented. As malignant primary and secondary brain tumors display a detrimental prognosis despite maximum treatment, detection of potential treatment targets at protein level is key for innovative future treatment approaches. This is especially important for clinical situations in which patients suffer from recurrent tumors with potentially new tumor-related pathways that might be newly activated in the context of treatment resistance. Buehler et al. address this topic by performing proteomic profiling of primary and recurrent glioblastomas deriving from 42 patients of two different clinical cohorts [8]. Of note, the applied proteomic analysis is equally suitable for frozen and formalin-fixed, paraffin-embedded (FFPE) tissues, the latter facilitating its applicability in diagnostic pathology [22]. In general, the proteomes of the initial glioblastomas as compared to their recurrent counterparts were highly similar, however, several proteins were significantly enriched in recurrences, including, among others, brain enriched myelin associated protein 1 (BCAS1), inverted formin 2 (INF2), calcium-calmodulin-dependent protein kinase 2 (CaMK2), phosphoribosyl pyrophosphate synthetase 2 (PRPS2) and F-Box only protein 2 (FBXO2). These results show that the method is able to detect tumor progression-associated changes in FFPE tissue. The authors proceeded in validating an overexpression for BCAS2, INF2 and FBXO2 in recurrent glioblastoma by means of immunohistochemistry and RNA sequencing. Regarding the clinical impact of those findings, significantly lower expression levels for INF2 and FBXO2 were found in glioblastoma patients with longer survival rates, therefore indicating that both factors might be implicated in tumor progression or treatment-resistance mechanisms. Using a murine approach, the authors could validate the survival benefit in FBXO2 knockout conditions, as well as showing a reduced tumor cell growth and invasive behavior in organotypic brain tumor slice cultures. While the authors focus more on addressing the role of FBXO2 activation as a driver for glioblastoma progression and recurrence at the end of their paper, I would rather stress the potential of the method for personalized medicine approaches in the future. Taking into account a) the horrible clinical prognosis of glioblastoma patients, b) the poor treatment options at the time of glioblastoma recurrence and c) that data derived from large-scale DNA or RNA analyses do not unequivocally predict the functional proteomic landscape, deciphering active tumor-related pathways by proteomic approaches in a close to routine pathological setting could be a great asset especially for recurrent tumors as compared to their primary counterparts. It would be of interest to run proteomic analyses much more frequently in parallel to large-scale genetic screenings, which could help to support decision making in molecular tumor boards. 7. Methylome-based brain tumor diagnostics in CSF liquid biopsies [9] Since neurosurgical interventions are among the most invasive medical procedures, the threshold to perform a brain biopsy is high. Avoiding biopsies for brain tumor types in which no subsequent resection would be performed (e.g. lymphomas) or that would significantly benefit from maximum resection would be highly desirable. With their approach to diagnose brain tumors by methylation analyses from cerebrospinal fluid (CSF) samples, Zuccato et al. pave the way for a less invasive, still highly reliable liquid-based brain tumor classification [9]. In this pioneering approach necessitating only very small amounts of CSF, the authors analyzed 57 brain metastases, glioblastomas and central nervous system lymphomas. A largely similar amount of cell-free DNA was obtained from CSF samples of all 3 tumor classes. The methylation profile significantly correlated between CSF and tumor samples in all 3 tumor entities. Furthermore, the methylation analyses could convincingly distinguish between brain metastases, glioblastoma and CNS lymphoma. The methylation profiles of CNS lymphomas were highly discriminatory. Therefore, perioperative morbidity and mortality could be considerably reduced in the future if such a CSF based methylation approach would be implemented in the routine diagnostic set-up before the final decision to perform gross resection is made. The prediction from methylation data in the present study was superior as compared to previously published data using plasma samples, which could be related to the closer proximity of brain tumors to the sampled CSF and the distribution of cell-free DNA in less volume with less liquid turnover as compared to plasma samples [23, 24]. In addition to the very promising findings regarding initial diagnostics of a primary tumor, this approach has also a high potential to track treatment responses or detect recurrent tumor cell growth. The strong correlation between primary tumors and CSF samples might also be useful to differentiate a primary brain tumor from metastasis in patients suffering from different cancer entities at the same time. 8. Intraoperative diagnostics for brain tumors based on Raman effect [10, 11] Intraoperative brain tumor diagnostics necessitate an availability of experienced neuropathologists, however, multiple smaller centers have only one or none of this rather rare “species”. Furthermore, diagnostic quality and precision may be suboptimal and frequently show less than 70% complete concordance with final neuropathological diagnoses [25]. Therefore, the central intraoperative questions are rather if the neurosurgeon correctly hit the lesion or if enough material was obtained for further microscopic and molecular diagnostics. Taking all those arguments into account, there is an obvious need for faster, more unbiased, less work intensive and, ideally, automated intraoperative diagnostic procedures. It was shown that label-free, stimulated Raman based histology (SRH) assessed by machine learning algorithms was able to provide an intraoperative diagnosis almost in real-time without showing less diagnostic precision as compared to experienced pathologists [26]. This method is based on the Raman scattering effect, namely, that the energy level of light can be altered upon interaction with molecular bonds, changes that can be visualized spectrophotometrically only [for comprehensive overview, please see 27]. When this method iscombined with a microscopic device, a spatial resolution between 0.5 and 1µm is achieved. Reinecke et al. applied SRH on a larger series of intraoperative neuro-oncological cases and created an automated diagnostic pipeline based on convolutional neural network analyses, revealing a high diagnostic accuracy as compared to an independently performed neuropathological assessment [11]. Furthermore, a high consistency between randomly chosen areas on tumor samples was observed. Taking into account that decision from this automated diagnostic pipeline took less than 5 minutes in total, this approach seems to be highly promising to replace intraoperative neuropathological intervention in the medium term. As especially pediatric brain tumors are nowadays much more specifically classified according to molecular pathological markers, microscopic diagnostics during surgery is frequently of limited value if intraoperative statement is, for example, “small round blue cell tumor” or “suspicion of low-grade glioma”. If a fast unbiased intraoperative method would be able to distinguish normal from tumor tissue and high from lower grade brain tumors in addition to a good estimation of the tumor cell content, this would considerably decrease the need for neuropathology expertise during the surgical procedure. In particular, the presence or absence of tumoris strongly needed information during the surgical procedure, as the extent of resection is one the most important predictors for progression free survival in pediatric brain tumors [28] Jabarkheel et al. investigated the suitability of Raman spectroscopy for pediatric brain tumor cases [10]. With their approach, Jabarkheel et al. were able to correctly distinguish tumor tissue from normal tissue in 89.9%; furthermore, the more complicated task of differentiating low-grade tumors from normal brain tissue was mastered in 86.2%. Although this development may impact neuropathology as a gold standard in intraoperative brain tumor diagnostics (Figure 3), neuropathologists are still key for the further development of these approaches as well-functioning machine learning pipelines need an excellent prior histological and molecular annotation.
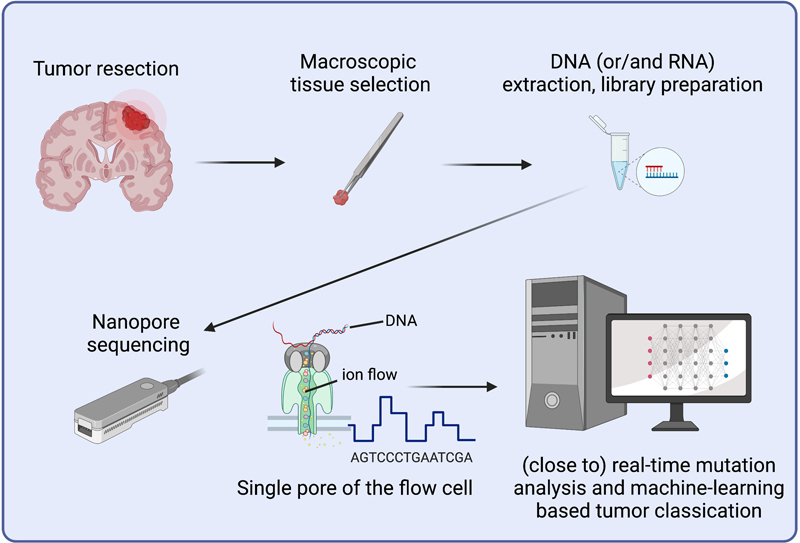
Figure 3: Potential intraoperative applications of Raman effect-based techniques combined with machine learning tools. Raman spectroscopy is a label-free, non-disruptive method based on an inelastic scattering effect of photons allowing for the quantitative molecular assessment of biological samples resulting in different spectra. Stimulated Raman histology (SRH) is a variant of Raman spectroscopy allowing for the creation of hematoxylin and eosin (HE) slide mimics based on quantification of distinct molecules (mainly lipids, proteins and nucleic acids). 9. Intraoperative molecular tumor profiling [12, 13] Molecular diagnostics becomes more and more important not only for precise patient stratification but also for targeted therapy strategies [29]. Especially in the field of CNS neoplasms, some entities can nowadays only be unequivocally diagnosed by methylation profiling [20]. Along this line, technical developments and applications related to molecular tumor testing need to take into account diagnostic precision, speed and costs. As the Method of the Year 2022, Nature Methods has chosen long-read sequencing, with Single Molecule Real-Time (SMRT) from Pacific Biosciences and nanopore sequencing (NPS) from Oxford Nanopore Technologies being the most frequently used commercially available applications [30]. While accuracy seems to be only slightly superior in SMRT as compared to NPS, the latter allows for longer average read lengths (approximately 100kb for ultra-long reads) as compared to SMRT. It is therefore no surprise that those techniques could also have an impact on diagnostic strategies in neuropathological tumor diagnostics. Using nanopore sequencing techniques, Patel et al. introduce a diagnostic pipeline entitled Rapid-CNS2 allowing for testing copy-number, mutational and methylation profiling in parallel [13]. With this approach, considerably simplified library preparations at lower costs are possible with highly similar diagnostic precision as compared to standard methods (Figure 4). Discrepancies in isolated cases were related to a low tumor cell content, therefore, a careful standard microscopic neuropathological assessment is mandatory during the workflow. A pure sequencing time of 24 hours was sufficient to conclude cases with a comprehensive neuropathological diagnosis, however, this pipeline is currently restricted in use for cryo-preserved tissue only. In a similar nanopore sequencing approach, however, focusing on methylation profiling without having the full molecular profile for important selected mutations, Kuschel et al. performed a combined retro- and prospective study arriving at a total turnaround time of only 21 hours from sample reception to report of the diagnoses [12]. Of note, as few as 1000 randomly analyzed CpGs were sufficient for highly meaningful methylation classification. Multiple initiatives are ongoing, pushing even further towards direct intraoperative molecular tumor profiling [31]. As final treatment decisions according to standard treatment guidelines are often made only several days after the operation in multidisciplinary tumor boards, one could question the necessity of speeding up intraoperative diagnostic assessments. However, as multiple innovative, targeted anti-tumor treatment approaches such as the application of T cells harboring chimeric antigen receptors (CAR-T cells) or oncolytic viruses would necessitate a follow-up neurosurgical intervention, e.g. for the placement of a catheter after the exact molecular definition of potential targets, intraoperative tumor diagnostics could overcome those obstacles.
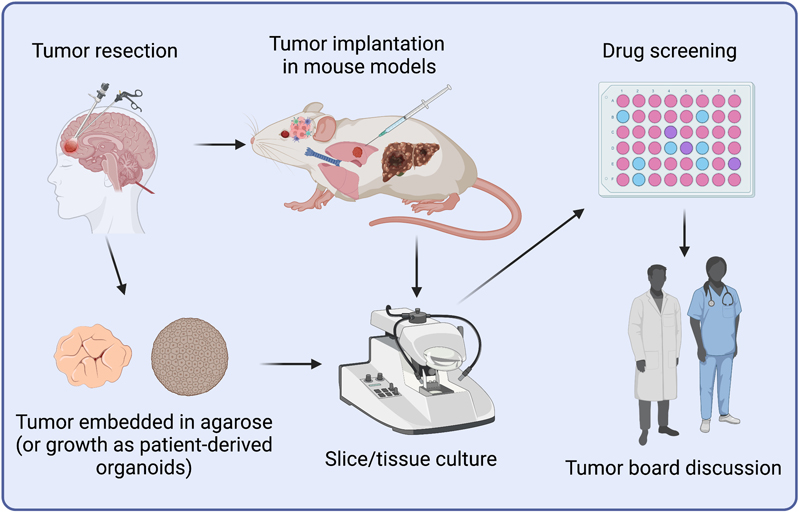
Figure 4: Scheme for fast, precise and unbiased molecular diagnostics using Nanopore sequencing, suitable for mutational, transcriptome and methylome analyses. 10. Drug screening platform for brain metastasis [14] Brain metastases constitute the group of the most frequent and malignant brain tumors that may affect around 20-25% of all cancer patients and are usually associated with a very poor prognosis [32, 33]. Although brain metastases comprise a very heterogenous group regarding their cellular origin, the site of metastasis as well as the number of metastatic spots, in many clinical conditions no entity- or target-specific treatment is available. Furthermore, even though both primary and secondary tumors are more and more profiled by means of molecular diagnostics, potential molecular targets might be no longer successfully druggable as the development of resistance mechanisms may negatively impact targeted treatment. To overcome these drawbacks, drug screening platforms are emerging that may allow for deciphering the best drugs specifically applicable for individual brain metastasis in a preclinical or clinical setting (Figure 5). Zhu et al. developed a murine model giving rise to brain metastasis upon tumor cell injection in the left heart ventricle [14]. From those animals, organotypic slice cultures of brain metastases were performed and treated with a drug-library consisting of 114 drugs, that were either FDA-approved or are currently in use in clinical trials. The use of slice culture has the advantage that tumor cells can grow in their associated microenvironment which is key for both the metastasizing process, but may also play an important role in treatment resistance. With this so-called medium-throughput drug-screening platform (METPlatform), they were able to identify a blood-barrier permeable HSP90 inhibitor as a promising drug for the treatment of brain metastases. In a follow-up experiment, the authors successfully treated patient-derived organotypic cultures deriving from various different cancer types. While the paper was focusing more on elucidating the underlying mechanisms of HSP90 inhibition in brain metastasis treatment, targeting HSP90 will certainly once again not be suitable as a “one fits all” in future brain metastasis treatment. What could be much more important in the future, is to make use of METPlatform or other similar drug-testing pipelines as a clinical “avatar”, as the authors called their approach. With this, medium or even high-throughput drug libraries could be applied on either primary tumor slices or tumor-derived organoids with the goal to individually decipher the most promising treatment strategies for this most detrimental clinical situation. Although slice culture-based approaches seem to excellently reflect the microenvironmental composition of the tumor in situ, the high variability between slices as well as the potentially limited availability of consecutive slices may negatively impact a homogenous readout when using larger drug libraries. This potential drawback could be potentially overcome by creating ex-vivo spheroids as an alternative “avatar”, that have already shown their clinical suitability in single patients with metastatic tumors [34].
Figure 5: Potential implementation of personalized drug-screening approaches in the clinical setting. Discussion This overview regarding key developments of the year 2022 in the field of neuro-oncology (with a link to neuropathology) clearly shows that scientific findings are very closely linked to technical developments. Nanopore sequencing has been proposed as one of the methods of the year 2022 [30] by Nature Methods as it allows for faster, unbiased, precise diagnostics having the advantage of assessing mutations, transcriptome and methylome by using only one device at relatively low costs. It is, therefore, no wonder that multiple initiatives have started to apply such techniques seeing a potential to provide intraoperative molecular diagnostics [12, 13]. In some clinical disciplines such as gynecological oncology [35], more and more molecular tests are commercialized in a highly protected manner, especially if it comes to prognostic prediction for distinct treatment regimens. In contrast, the neuropathology community – at least until now – has managed to keep complex diagnostic tests running within the scientific community for a long time without commercialization [15]. Those initiatives, mainly based on excellent clinical data, neuropathological annotations and research-driven modeling and machine learning, were mostly financed by governmental support or funding organizations and have frequently proven their high value for the healthcare system, e.g. by dramatically changing the most recent WHO classification [20]. It remains to be determined how those approaches can sustainably be kept running, for example by hosting joint platforms openly accessible on university servers. Another potential risk is the fact that several machine learning approaches are based on data mainly deriving from a specific platform (e.g. Illumina Infinium MethylationEPIC Array ®) and would need new validation when new techniques for the same application are coming on the market (e.g. changing from Array-based methylome to Nanopore sequencing). This could even affect the WHO classification as several tumor entities are currently essentially defined by their methylation profile, such as high-grade astrocytoma with piloid features, astroblastoma with MN1 alteration, diffuse glioneuronal tumour with oligodendroglioma-like features and nuclear clusters (DGONC) or papillary glioneuronal tumor, while for many others the methylation profile is included as a desirable diagnostic criterion [20]. The use of joint worldwide platforms also has the advantage to discover much faster new, rare tumor entities as it has been successfully shown in 2022 with high-grade glioma with pleomorphic and pseudopapillary features (HPAP), an entity that would otherwise have been associated with a wrong prognostic prediction if diagnosis would have been based on classic microscopic assessment only [3]. Along this line, the WHO has an important role in balancing between the clinical needs in underdeveloped countries and the amazing advances that especially come up in first world academic centers in the field of molecular tumor profiling. It is therefore as important to continue with finding simple diagnostic tools for exact prognostic or therapeutic prediction as presented for the prediction of the 1p/19q status in IDH-mutant glioma by an easy 2-step IHC-based approach [4]. If machine learning algorithms for microscopic (neuro-)pathological assessments would be as powerful as shown for molecular pathology or radiology [36], the latter now even aiming for quantitative analyses, new histology-based classification algorithms would then allow for a very cheap assessment of HE slides in underdeveloped countries. Therefore, the study of Liechty et al. has also been selected as a highlight as it shows that machine learning-based diagnostics may be similarly powerful as a (neuro-)pathologist [5]. Such an approach could be helpful not only for countries where no neuropathologists are available, but also for smaller health care centers, in which a 4 (or more) eye principle is not possible. The fact that “artificial intelligence” never gets tired and is able to quickly capture information from huge databases, a task for which an experienced pathologist would need decades, may be very worrying for classic “histomorphologists”. This might be even more the case when machine-learning pipelines will be more directly fed with clinical, radiological and molecular data. Nowadays, it is already very clear that morphological classification alone is significantly inferior to approaches that also take into account molecular pathological data [6]. As previously shown for several joint initiatives in molecular profiling, it would be highly beneficial if prognostic prediction algorithms would be cross-validated with the goal to constantly improve, instead of having several competing grading systems [6, 17]. Similarly, joint efforts would of course be necessary for other ongoing initiatives that have been presented in this manuscript, such as methylome-based brain tumor diagnostics in CSF liquid biopsies [9], molecular profiling for entities that are not yet broadly covered in openly accessible classification pipelines, [7] or more recently upcoming techniques such as close to real-time diagnostic approaches based on the Raman effect [10, 11]. While most profiling studies published in 2022 rather focused on “faster, deeper, broader, more precise”, really new concepts were very infrequently encountered. One very interesting approach is based on a deciphering the proteomic landscape in recurrent glioblastoma as compared to its primary counterpart [8]. This method would allow for a personalized treatment addressing potentially newly activated tumor pathways emerging during treatment resistance and recurrence. Focusing on the tumor-associated proteome, one may get more real functional information about the tumor cells as compared to transcriptome, methylome or mutational analyses. Finally, it is of high importance to come up with new, more personalized treatment approaches, especially for patients suffering from recurrent malignant brain tumors with a detrimental prognosis for which no really helpful established treatment schemes are available. A promising approach is the use of drug screening libraries which may be very useful to detect potential drugs that cannot easily be predicted by deep sequencing analyses [14]. As the author put the brain tumor cell(s) in the center of this “top ten” series, several high impact papers that focused on cells of or interaction mechanisms within the tumor microenvironment unfortunately did not make it on this list. An amazing new concept about how glioblastoma cells are hijacking neuronal activity for invasion has been presented, however, it remains to be determined to which degree this is important in humans and if this mechanism may serve as a potential future treatment target [37]. Another fascinating study showed in a murine model that a loss of MHC-II on blood-borne myeloid cells leads to dysfunctional CD8-positive cytotoxic T cells and therefore impaired tumor control while functional MHC-II-restricted antigen presentation was associated with improved tumor control [38]. Although the authors could show an inverse correlation of MHC-II expression with dysfunctional CD8-positive T cell phenotypes, this finding was only provided in a very small cohort of human glioblastoma samples and needs further corroboration. In conclusion, neurooncological research in 2022 provided a huge number of excellent studies that considerably improved speed and precision in classifying tumors of the central nervous system, detected new tumor entities and provided promising approaches for more individualized treatment approaches. There is nothing else for it but to hope that at least some of those approaches finally make it into a therapeutic application thereby helping to improve the still detrimental prognosis of patients with malignant brain tumors. Acknowledgements MM would like to thank the Luxembourg National Research Fond (FNR) for the support (FNR PEARL P16/BM/11192868 grant). The figures were prepared using https://biorender.com figure creation tool. Single images using for the figures were freely available tagged with creative common license. Declaration of Interests The author declares to not have any competing interests. References 1. Falagas ME, Pitsouni EI, Malietzis GA, Pappas G. Comparison of PubMed, Scopus, Web of Science, and Google Scholar: strengths and weaknesses. FASEB J. 2008 Feb;22(2):338-42. https://doi.org/10.1096/fj.07-9492LSF. Epub 2007 Sep 20. PMID: 17884971. 2. Shariff SZ, Bejaimal SA, Sontrop JM, Iansavichus AV, Haynes RB, Weir MA, Garg AX. Retrieving clinical evidence: a comparison of PubMed and Google Scholar for quick clinical searches. J Med Internet Res. 2013 Aug 15;15(8):e164. https://doi.org/10.2196/jmir.2624. PMID: 23948488. 3. Pratt D, Abdullaev Z, Papanicolau-Sengos A, Ketchum C, Panneer Selvam P, Chung HJ, Lee I, Raffeld M, Gilbert MR, Armstrong TS, Pytel P, Borys E, Klonoski JM, McCord M, Horbinski C, Brat D, Perry A, Solomon D, Eberhart C, Giannini C, Quezado M, Aldape K. High-grade glioma with pleomorphic and pseudopapillary features (HPAP): a proposed type of circumscribed glioma in adults harboring frequent TP53 mutations and recurrent monosomy 13. Acta Neuropathol. 2022 Mar;143(3):403-414. https://doi.org/10.1007/s00401-022-02404-9. Epub 2022 Feb 1. PMID: 35103816. 4. Felix M, Friedel D, Jayavelu AK, Filipski K, Reinhardt A, Warnken U, Stichel D, Schrimpf D, Korshunov A, Wang Y, Kessler T, Etminan N, Unterberg A, Herold-Mende C, Heikaus L, Sahm F, Wick W, Harter PN, von Deimling A, Reuss DE. HIP1R and vimentin immunohistochemistry predict 1p/19q status in IDH-mutant glioma. Neuro Oncol. 2022 Dec 1;24(12):2121-2132. https://doi.org/10.1093/neuonc/noac111. PMID: 35511748. 5. Liechty B, Xu Z, Zhang Z, Slocum C, Bahadir CD, Sabuncu MR, Pisapia DJ. Machine learning can aid in prediction of IDH mutation from H&E-stained histology slides in infiltrating gliomas. Sci Rep. 2022 Dec 31;12(1):22623. https://doi.org/10.1038/s41598-022-26170-6. PMID: 36587030. 6. Driver J, Hoffman SE, Tavakol S, Woodward E, Maury EA, Bhave V, Greenwald NF, Nassiri F, Aldape K, Zadeh G, Choudhury A, Vasudevan HN, Magill ST, Raleigh DR, Abedalthagafi M, Aizer AA, Alexander BM, Ligon KL, Reardon DA, Wen PY, Al-Mefty O, Ligon AH, Dubuc AM, Beroukhim R, Claus EB, Dunn IF, Santagata S, Linda Bi W. A molecularly integrated grade for meningioma. Neuro Oncol. 2022 May 4;24(5):796-808. https://doi.org/10.1093/neuonc/noab213. PMID: 34508644. 7. Radke J, Ishaque N, Koll R, Gu Z, Schumann E, Sieverling L, Uhrig S, Hübschmann D, Toprak UH, López C, Hostench XP, Borgoni S, Juraeva D, Pritsch F, Paramasivam N, Balasubramanian GP, Schlesner M, Sahay S, Weniger M, Pehl D, Radbruch H, Osterloh A, Korfel A, Misch M, Onken J, Faust K, Vajkoczy P, Moskopp D, Wang Y, Jödicke A, Trümper L, Anagnostopoulos I, Lenze D, Küppers R, Hummel M, Schmitt CA, Wiestler OD, Wolf S, Unterberg A, Eils R, Herold-Mende C, Brors B; ICGC MMML-Seq Consortium; Siebert R, Wiemann S, Heppner FL. The genomic and transcriptional landscape of primary central nervous system lymphoma. Nat Commun. 2022 May 10;13(1):2558. https://doi.org/10.1038/s41467-022-30050-y. PMID: 35538064. 8. Buehler M, Yi X, Ge W, Blattmann P, Rushing E, Reifenberger G, Felsberg J, Yeh C, Corn JE, Regli L, Zhang J, Cloos A, Ravi VM, Wiestler B, Heiland DH, Aebersold R, Weller M, Guo T, Weiss T. Quantitative proteomic landscapes of primary and recurrent glioblastoma reveal a protumorigeneic role for FBXO2-dependent glioma-microenvironment interactions. Neuro Oncol. 2023 Feb 14;25(2):290-302. https://doi.org/10.1093/neuonc/noac169. PMID: 35802605. 9. Zuccato JA, Patil V, Mansouri S, Voisin M, Chakravarthy A, Shen SY, Nassiri F, Mikolajewicz N, Trifoi M, Skakodub A, Zacharia B, Glantz M, De Carvalho DD, Mansouri A, Zadeh G. Cerebrospinal fluid methylome-based liquid biopsies for accurate malignant brain neoplasm classification. Neuro Oncol. 2022 Dec 1:noac264. https://doi.org/10.1093/neuonc/noac264. Online ahead of print. PMID: 36455236. 10. Jabarkheel R, Ho CS, Rodrigues AJ, Jin MC, Parker JJ, Mensah-Brown K, Yecies D, Grant GA. Rapid intraoperative diagnosis of pediatric brain tumors using Raman spectroscopy: A machine learning approach. Neurooncol Adv. 2022 Jul 26;4(1):vdac118. https://doi.org/10.1093/noajnl/vdac118. eCollection 2022 Jan-Dec. PMID: 35919071. 11. Reinecke D, von Spreckelsen N, Mawrin C, Ion-Margineanu A, Fürtjes G, Jünger ST, Khalid F, Freudiger CW, Timmer M, Ruge MI, Goldbrunner R, Neuschmelting V. Novel rapid intraoperative qualitative tumor detection by a residual convolutional neural network using label-free stimulated Raman scattering microscopy. Acta Neuropathol Commun. 2022 Aug 6;10(1):109. https://doi.org/10.1186/s40478-022-01411-x. PMID: 35933416. 12. Kuschel LP, Hench J, Frank S, Hench IB, Girard E, Blanluet M, Masliah-Planchon J, Misch M, Onken J, Czabanka M, Yuan D, Lukassen S, Karau P, Ishaque N, Hain EG, Heppner F, Idbaih A, Behr N, Harms C, Capper D, Euskirchen P. Robust methylation-based classification of brain tumours using nanopore sequencing. Neuropathol Appl Neurobiol. 2023 Feb;49(1):e12856. https://doi.org/10.1111/nan.12856. PMID: 36269599. 13. Patel A, Dogan H, Payne A, Krause E, Sievers P, Schoebe N, Schrimpf D, Blume C, Stichel D, Holmes N, Euskirchen P, Hench J, Frank S, Rosenstiel-Goidts V, Ratliff M, Etminan N, Unterberg A, Dieterich C, Herold-Mende C, Pfister SM, Wick W, Loose M, von Deimling A, Sill M, Jones DTW, Schlesner M, Sahm F. Rapid-CNS2: rapid comprehensive adaptive nanopore-sequencing of CNS tumors, a proof-of-concept study. Acta Neuropathol. 2022 May;143(5):609-612. https://doi.org/10.1007/s00401-022-02415-6. Epub 2022 Mar 31. PMID: 35357562. 14. Zhu L, Retana D, García-Gómez P, Álvaro-Espinosa L, Priego N, Masmudi-Martín M, Yebra N, Miarka L, Hernández-Encinas E, Blanco-Aparicio C, Martínez S, Sobrino C, Ajenjo N, Artiga MJ, Ortega-Paino E, Torres-Ruiz R, Rodríguez-Perales S; RENACER; Soffietti R, Bertero L, Cassoni P, Weiss T, Muñoz J, Sepúlveda JM, González-León P, Jiménez-Roldán L, Moreno LM, Esteban O, Pérez-Núñez Á, Hernández-Laín A, Toldos O, Ruano Y, Alcázar L, Blasco G, Fernández-Alén J, Caleiras E, Lafarga M, Megías D, Graña-Castro O, Nör C, Taylor MD, Young LS, Varešlija D, Cosgrove N, Couch FJ, Cussó L, Desco M, Mouron S, Quintela-Fandino M, Weller M, Pastor J, Valiente M. A clinically compatible drug-screening platform based on organotypic cultures identifies vulnerabilities to prevent and treat brain metastasis. EMBO Mol Med. 2022 Mar 7;14(3):e14552. https://doi.org/10.15252/emmm.202114552. Epub 2022 Feb 17. PMID: 35174975. 15. Capper D, Jones DTW, Sill M, Hovestadt V, Schrimpf D, Sturm D, Koelsche C, Sahm F, Chavez L, Reuss DE, Kratz A, Wefers AK, Huang K, Pajtler KW, Schweizer L, Stichel D, Olar A, Engel NW, Lindenberg K, Harter PN, Braczynski AK, Plate KH, Dohmen H, Garvalov BK, Coras R, Hölsken A, Hewer E, Bewerunge-Hudler M, Schick M, Fischer R, Beschorner R, Schittenhelm J, Staszewski O, Wani K, Varlet P, Pages M, Temming P, Lohmann D, Selt F, Witt H, Milde T, Witt O, Aronica E, Giangaspero F, Rushing E, Scheurlen W, Geisenberger C, Rodriguez FJ, Becker A, Preusser M, Haberler C, Bjerkvig R, Cryan J, Farrell M, Deckert M, Hench J, Frank S, Serrano J, Kannan K, Tsirigos A, Brück W, Hofer S, Brehmer S, Seiz-Rosenhagen M, Hänggi D, Hans V, Rozsnoki S, Hansford JR, Kohlhof P, Kristensen BW, Lechner M, Lopes B, Mawrin C, Ketter R, Kulozik A, Khatib Z, Heppner F, Koch A, Jouvet A, Keohane C, Mühleisen H, Mueller W, Pohl U, Prinz M, Benner A, Zapatka M, Gottardo NG, Driever PH, Kramm CM, Müller HL, Rutkowski S, von Hoff K, Frühwald MC, Gnekow A, Fleischhack G, Tippelt S, Calaminus G, Monoranu CM, Perry A, Jones C, Jacques TS, Radlwimmer B, Gessi M, Pietsch T, Schramm J, Schackert G, Westphal M, Reifenberger G, Wesseling P, Weller M, Collins VP, Blümcke I, Bendszus M, Debus J, Huang A, Jabado N, Northcott PA, Paulus W, Gajjar A, Robinson GW, Taylor MD, Jaunmuktane Z, Ryzhova M, Platten M, Unterberg A, Wick W, Karajannis MA, Mittelbronn M, Acker T, Hartmann C, Aldape K, Schüller U, Buslei R, Lichter P, Kool M, Herold-Mende C, Ellison DW, Hasselblatt M, Snuderl M, Brandner S, Korshunov A, von Deimling A, Pfister SM. DNA methylation-based classification of central nervous system tumours. Nature. 2018 Mar 22;555(7697):469-474. https://doi.org/10.1038/nature26000. Epub 2018 Mar 14. PMID: 29539639. 16. Raffeld M, Abdullaev Z, Pack SD, Xi L, Nagaraj S, Briceno N, Vera E, Pittaluga S, Lopes Abath Neto O, Quezado M, Aldape K, Armstrong TS, Gilbert MR. High level MYCN amplification and distinct methylation signature define an aggressive subtype of spinal cord ependymoma. Acta Neuropathol Commun. 2020 Jul 8;8(1):101. https://doi.org/10.1186/s40478-020-00973-y. PMID: 32641156. 17. Sahm F, Schrimpf D, Stichel D, Jones DTW, Hielscher T, Schefzyk S, Okonechnikov K, Koelsche C, Reuss DE, Capper D, Sturm D, Wirsching HG, Berghoff AS, Baumgarten P, Kratz A, Huang K, Wefers AK, Hovestadt V, Sill M, Ellis HP, Kurian KM, Okuducu AF, Jungk C, Drueschler K, Schick M, Bewerunge-Hudler M, Mawrin C, Seiz-Rosenhagen M, Ketter R, Simon M, Westphal M, Lamszus K, Becker A, Koch A, Schittenhelm J, Rushing EJ, Collins VP, Brehmer S, Chavez L, Platten M, Hänggi D, Unterberg A, Paulus W, Wick W, Pfister SM, Mittelbronn M, Preusser M, Herold-Mende C, Weller M, von Deimling A. DNA methylation-based classification and grading system for meningioma: a multicentre, retrospective analysis. Lancet Oncol. 2017 May;18(5):682-694. https://doi.org/10.1016/S1470-2045(17)30155-9. Epub 2017 Mar 15. PMID: 28314689. 18. Wesseling P, Rozowsky JS. Neurooncology: 2022 update. Free Neuropathology 3:4. 2022. https://doi.org/10.17879/freeneuropathology-2022-3804/. 19. Hielscher T, Sill M, Sievers P, Stichel D, Brandner S, Jones DTW, von Deimling A, Sahm F, Maas SLN. Clinical implementation of integrated molecular-morphologic risk prediction for meningioma. Brain Pathol. 2022 Nov 14:e13132. https://doi.org/10.1111/bpa.13132. Online ahead of print. PMID: 36377252. 20. World Health Organization Classification of Tumours of the Central Nervous System. 5th ed.Lyon: International Agency for Research on Cancer; 2021. 21. Fangazio M, Ladewig E, Gomez K, Garcia-Ibanez L, Kumar R, Teruya-Feldstein J, Rossi D, Filip I, Pan-Hammarström Q, Inghirami G, Boldorini R, Ott G, Staiger AM, Chapuy B, Gaidano G, Bhagat G, Basso K, Rabadan R, Pasqualucci L, Dalla-Favera R. Genetic mechanisms of HLA-I loss and immune escape in diffuse large B cell lymphoma. Proc Natl Acad Sci U S A. 2021 Jun 1;118(22):e2104504118. https://doi.org/10.1073/pnas.2104504118. PMID: 34050029. 22. Zhu Y, Weiss T, Zhang Q, Sun R, Wang B, Yi X, Wu Z, Gao H, Cai X, Ruan G, Zhu T, Xu C, Lou S, Yu X, Gillet L, Blattmann P, Saba K, Fankhauser CD, Schmid MB, Rutishauser D, Ljubicic J, Christiansen A, Fritz C, Rupp NJ, Poyet C, Rushing E, Weller M, Roth P, Haralambieva E, Hofer S, Chen C, Jochum W, Gao X, Teng X, Chen L, Zhong Q, Wild PJ, Aebersold R, Guo T. High-throughput proteomic analysis of FFPE tissue samples facilitates tumor stratification. Mol Oncol. 2019 Nov;13(11):2305-2328. https://doi.org/10.1002/1878-0261.12570. Epub 2019 Sep 18. PMID: 31495056. 23. Nassiri F, Chakravarthy A, Feng S, Shen SY, Nejad R, Zuccato JA, Voisin MR, Patil V, Horbinski C, Aldape K, Zadeh G, De Carvalho DD. Detection and discrimination of intracranial tumors using plasma cell-free DNA methylomes. Nat Med. 2020 Jul;26(7):1044-1047. https://doi.org/10.1038/s41591-020-0932-2. Epub 2020 Jun 22. PMID: 32572265. 24. Shen SY, Singhania R, Fehringer G, Chakravarthy A, Roehrl MHA, Chadwick D, Zuzarte PC, Borgida A, Wang TT, Li T, Kis O, Zhao Z, Spreafico A, Medina TDS, Wang Y, Roulois D, Ettayebi I, Chen Z, Chow S, Murphy T, Arruda A, O'Kane GM, Liu J, Mansour M, McPherson JD, O'Brien C, Leighl N, Bedard PL, Fleshner N, Liu G, Minden MD, Gallinger S, Goldenberg A, Pugh TJ, Hoffman MM, Bratman SV, Hung RJ, De Carvalho DD. Sensitive tumour detection and classification using plasma cell-free DNA methylomes. Nature. 2018 Nov;563(7732):579-583. https://doi.org/10.1038/s41586-018-0703-0. Epub 2018 Nov 14. PMID: 30429608. 25. Yadav M, Sharma P, Singh V, Tewari R, Mishra PS, Roy K. An Audit of Diagnostic Disparity between Intraoperative Frozen Section Diagnosis and Final Histopathological Diagnosis of Central Nervous System Lesions at a Tertiary Care Center. J Lab Physicians. 2022 Aug 17;14(4):384-393. https://doi.org/10.1055/s-0042-1750064. eCollection 2022 Dec. PMID: 36531541. 26. Hollon TC, Pandian B, Adapa AR, Urias E, Save AV, Khalsa SSS, Eichberg DG, D'Amico RS, Farooq ZU, Lewis S, Petridis PD, Marie T, Shah AH, Garton HJL, Maher CO, Heth JA, McKean EL, Sullivan SE, Hervey-Jumper SL, Patil PG, Thompson BG, Sagher O, McKhann GM 2nd, Komotar RJ, Ivan ME, Snuderl M, Otten ML, Johnson TD, Sisti MB, Bruce JN, Muraszko KM, Trautman J, Freudiger CW, Canoll P, Lee H, Camelo-Piragua S, Orringer DA. Near real-time intraoperative brain tumor diagnosis using stimulated Raman histology and deep neural networks. Nat Med. 2020 Jan;26(1):52-58. https://doi.org/10.1038/s41591-019-0715-9. Epub 2020 Jan 6. PMID: 31907460. 27. Klamminger GG, Frauenknecht K, Mittelbronn M, Kleine Borgmann FB. From Research to Diagnostic Application of Raman Spectroscopy in Neurosciences: Past and Perspectives. 2022. Free Neuropathology, 3, 19. https://doi.org/10.17879/freeneuropathology-2022-4210. 28. Wisoff JH, Sanford RA, Heier LA, Sposto R, Burger PC, Yates AJ, Holmes EJ, Kun LE. Primary neurosurgery for pediatric low-grade gliomas: a prospective multi-institutional study from the Children's Oncology Group. Neurosurgery. 2011 Jun;68(6):1548-54; discussion 1554-5. https://doi.org/10.1227/NEU.0b013e318214a66e. PMID: 21368693. 29. Jahn A, Rump A, Widmann TJ, Heining C, Horak P, Hutter B, Paramasivam N, Uhrig S, Gieldon L, Drukewitz S, Kübler A, Bermudez M, Hackmann K, Porrmann J, Wagner J, Arlt M, Franke M, Fischer J, Kowalzyk Z, William D, Weth V, Oster S, Fröhlich M, Hüllein J, Valle González C, Kreutzfeldt S, Mock A, Heilig CE, Lipka DB, Möhrmann L, Hanf D, Oleś M, Teleanu V, Allgäuer M, Ruhnke L, Kutz O, Knurr A, Laßmann A, Endris V, Neumann O, Penzel R, Beck K, Richter D, Winter U, Wolf S, Pfütze K, Geörg C, Meißburger B, Buchhalter I, Augustin M, Aulitzky WE, Hohenberger P, Kroiss M, Schirmacher P, Schlenk RF, Keilholz U, Klauschen F, Folprecht G, Bauer S, Siveke JT, Brandts CH, Kindler T, Boerries M, Illert AL, von Bubnoff N, Jost PJ, Metzeler KH, Bitzer M, Schulze-Osthoff K, von Kalle C, Brors B, Stenzinger A, Weichert W, Hübschmann D, Fröhling S, Glimm H, Schröck E, Klink B. Comprehensive cancer predisposition testing within the prospective MASTER trial identifies hereditary cancer patients and supports treatment decisions for rare cancers. Ann Oncol. 2022 Nov;33(11):1186-1199. https://doi.org/10.1016/j.annonc.2022.07.008. Epub 2022 Aug 18. PMID: 35988656. 30. Method of the Year 2022: long-read sequencing. Nat Methods. 2023 Jan;20(1):1. https://doi.org/10.1038/s41592-022-01759-x. PMID: 36635552. 31. Djirackor L, Halldorsson S, Niehusmann P, Leske H, Capper D, Kuschel LP, Pahnke J, Due-Tønnessen BJ, Langmoen IA, Sandberg CJ, Euskirchen P, Vik-Mo EO. Intraoperative DNA methylation classification of brain tumors impacts neurosurgical strategy. Neurooncol Adv. 2021 Oct 10;3(1):vdab149. https://doi.org/10.1093/noajnl/vdab149. eCollection 2021 Jan-Dec. PMID: 34729487. 32. Aizer AA, Lamba N, Ahluwalia MS, Aldape K, Boire A, Brastianos PK, Brown PD, Camidge DR, Chiang VL, Davies MA, Hu LS, Huang RY, Kaufmann T, Kumthekar P, Lam K, Lee EQ, Lin NU, Mehta M, Parsons M, Reardon DA, Sheehan J, Soffietti R, Tawbi H, Weller M, Wen PY. Brain metastases: A Society for Neuro-Oncology (SNO) consensus review on current management and future directions. Neuro Oncol. 2022 Oct 3;24(10):1613-1646. https://doi.org/10.1093/neuonc/noac118. PMID: 35762249. 33. Sacks P, Rahman M. Epidemiology of Brain Metastases. Neurosurg Clin N Am. 2020 Oct;31(4):481-488. https://doi.org/10.1016/j.nec.2020.06.001. PMID: 32921345. 34. Kim H, El-Khoury V, Schulte N, Zhan T, Betge J, Cousin L, Felli E, Pessaux P, Ogier A, Opitz O, Ku B, Ebert MP, Kwon YJ. Personalized functional profiling using ex-vivo patient-derived spheroids points out the potential of an antiangiogenic treatment in a patient with a metastatic lung atypical carcinoid. Cancer Biol Ther. 2022 Dec 31;23(1):96-102. https://doi.org/10.1080/15384047.2021.2021042. PMID: 35193475. 35. Sinn P, Aulmann S, Wirtz R, Schott S, Marmé F, Varga Z, Lebeau A, Kreipe H, Schneeweiss A. Multigene Assays for Classification, Prognosis, and Prediction in Breast Cancer: a Critical Review on the Background and Clinical Utility. Geburtshilfe Frauenheilkd. 2013 Sep;73(9):932-940. https://doi.org/10.1055/s-0033-1350831. PMID: 24771945. 36. Rogers W, Thulasi Seetha S, Refaee TAG, Lieverse RIY, Granzier RWY, Ibrahim A, Keek SA, Sanduleanu S, Primakov SP, Beuque MPL, Marcus D, van der Wiel AMA, Zerka F, Oberije CJG, van Timmeren JE, Woodruff HC, Lambin P. Radiomics: from qualitative to quantitative imaging. Br J Radiol. 2020 Apr;93(1108):20190948. https://doi.org/10.1259/bjr.20190948. Epub 2020 Feb 26. PMID: 32101448. 37. Venkataramani V, Yang Y, Schubert MC, Reyhan E, Tetzlaff SK, Wißmann N, Botz M, Soyka SJ, Beretta CA, Pramatarov RL, Fankhauser L, Garofano L, Freudenberg A, Wagner J, Tanev DI, Ratliff M, Xie R, Kessler T, Hoffmann DC, Hai L, Dörflinger Y, Hoppe S, Yabo YA, Golebiewska A, Niclou SP, Sahm F, Lasorella A, Slowik M, Döring L, Iavarone A, Wick W, Kuner T, Winkler F. Glioblastoma hijacks neuronal mechanisms for brain invasion. Cell. 2022 Aug 4;185(16):2899-2917.e31. https://doi.org/10.1016/j.cell.2022.06.054. Epub 2022 Jul 31. PMID: 35914528. 38. Kilian M, Sheinin R, Tan CL, Friedrich M, Krämer C, Kaminitz A, Sanghvi K, Lindner K, Chih YC, Cichon F, Richter B, Jung S, Jähne K, Ratliff M, Prins RM, Etminan N, von Deimling A, Wick W, Madi A, Bunse L, Platten M. MHC class II-restricted antigen presentation is required to prevent dysfunction of cytotoxic T cells by blood-borne myeloids in brain tumors. Cancer Cell. 2023 Feb 13;41(2):235-251.e9. https://doi.org/10.1016/j.ccell.2022.12.007. PMID: 36638785.
Copyright: © 2023 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |