|
|
|
Free Neuropathology 1:15 (2020) |
|
Reflections |
|
Neuropathology through the ages – personal reflections: |
|
Herbert Budka |
|
Medical University Vienna |
|
Corresponding author: |
|
Submitted: 19 May 2020 Accepted: 25 May 2020 Copyedited by: Biswa Ramani Published: 04 June 2020 |
|
The author´s CV has been attached as electronic supplementary material: CV supplementary material |
|
Keywords: Neuropathology, Institute of Neurology Vienna, Personal reflections |
|
Contents
Introduction
If I have seen farther than others, it is because
If I have not seen as far as others, it is because At my current age of 73, the ability to see – somewhere into the mid-distance between the quotations above – has been shaped by mentors, colleagues, students and trainees, friends and family. I started to write this since the second week of the CoVID-19-related lockdown. Virtually nobody was seen outside, a bizarre experience that reminds me of my first memories as an infant in post-war occupied Vienna when people tried to avoid public encounters, particularly with patrolling Soviet soldiers. In mid-March 2020, nobody could foresee how the SARS-CoV2 pandemic would evolve. As my wife, an active hospital nurse, and our 12-year-old daughter at school had and have some risk to get infected, we agreed to temporarily separate. Now I stay in self-imposed isolation with our dog Gorry in a small rented apartment in the beautiful Vienna Woods. Like others who, during the present lockdown, have a chance to re-consider their way of life, I have ample time to reflect on my life and on neuropathology. I write this just based on my memories, as most of my written documents are either back in my home or have been destroyed after I retired from my directorship of the (Clinical) Institute of Neurology, formerly Neurological Institute (NI, Obersteiner Institute) in Vienna. Without doubt, the reader will detect in these memoirs the characteristic reminiscence bump of psychology, i. e. the strongest memories date back to adolescence and early adulthood, and emotionally positive memories dominate. However, I consider my whole professional life as extraordinary privilege to have done what I enjoyed most, having made many friends and met great personalities including true giants in medicine, science and research. Moreover, I believe to have witnessed the golden era of neuropathology, spanning from rather subjective interpretation of classical morphology to unprecedentedly detailed molecular diagnoses and fascinating understanding of aetiologies and pathogenesis of diseases of the nervous system. I will keep this fascination forever. My family had the almost obligatory migrant background of Viennese. Probably my later commitment for refugees and human rights was the subconscious recognition of that fact. My father’s Budka (meaning small hut or kiosk in Slavic languages) family originated from the double town of Cieszyn (in Polish) / Těšín (in Czech) or Teschen (in German), at the Polish-Czech border in Silesia, then part of the Austrian empire. My grandfather migrated to Vienna where my father was born. I have only faint memories of my grandfather – the most vivid one is an old photograph depicting him, with a huge moustache and in a typical knee-long body jersey next to a huge and heavy iron bike, as winner of an Austrian bicycling championship. Another memory is my first visit with him to the Prater entertainment park that had just re-opened. In a haunted house train taking us around many horrifying corners that I passed by firmly closing my eyes, a ghost took grandpa’s hat away. Grandpa became very angry and tried to hit the culprit ghost with his stick. I was greatly impressed by such courage – even against ghosts! – also resulting in getting the hat back at the entrance. My mother’s Panoš family had lived in Olomouc (in Czech) or Olmütz (in German) where she was born. Her father was a recognised expert of beer brewing, then as now a classical Czech talent, who became employed by the then well-known Nussdorf brewery in Vienna. My fondness for beer seems to be another subconscious recognition of my heritage. I was born in 1946 in a small village in Upper Austria where my parents had to relocate after WWII bombs had destroyed their home in Vienna. However, we returned to Vienna when I was 3, and rented an apartment in an area where most buildings had been either razed to the ground or heavily damaged. For a boy, this was paradise: the building debris of ruins just across the street was an ideal adventure playground for all kids of the neighbourhood, including slopes for first skiing attempts and sledging, hiding places to play “doctor” and have your first smoke – not cigarettes, of course, but twigs of elder bush. Retrospectively, I think we were extremely lucky not to have found one of the many explosive war relics. My father worked as a salesman, and compared to others we did relatively well in the 1950s. He was a highly talented piano and violin player, and I still retain recordings of his usual training in Bach and Beethoven sonatas that accompanied my school homework. Moreover, we had weekly visits of friends who played string quartets or piano trios with my father. At the end of his life, he suffered from Alzheimer’s disease (AD), and one striking experiment confirmed more recent findings in brain research that the musical reminiscence bump survives longest in AD and arises strong emotions: in the chronic care institution where my father finally lived, a piano was existing, and once I took my father, then already in a very advanced disease stage, had him sit down and put his hands on the keys. As in the old times, he started immediately to play flawlessly, starting with Bach, then Beethoven and finally switching into a more popular Viennese waltz. All other patients and visitors in the hall immediately stopped to talk and listened. After some two to three minutes, my father suddenly stopped and appeared to be confused what was going on. There was thundering applause, a final salute to this great musician, and tears were running down his face. He died soon thereafter. Unfortunately, I was much less gifted in musical instruments, but my father forced me to exercise every day at least for one hour, hoping to have me become a famous pianist that was his own but failed life vision. Always thinking of something else more interesting during my daily practicing lessons at the piano, I can still hear him shouting corrections like “C sharp, not C” at the doorstep when he entered the house after work. It took me several years to convince him to allow me to stop playing, a decision that I regret very much now. I would love to play Mozart or Beethoven like I did as a child, but the rigid enforcement by my father erased or blocked all former training imprints in my brain. According to the traditional role model, my mother stayed at home and took care of my elder sister Monika and me (Fig. 1). Moreover, she was a housewife in the famous Bohemian tradition, with a cookbook that she wrote by hand after recipes told by her mother, an apparently outstanding cook. I am still hunting for that old Bohemian cookbook in our family records, as I have become more and more interested in perfecting my own cooking.
Fig. 1. The family in the mid-1950s. My father was also a good tennis player, and with tennis he was more successful to get me interested than with the piano. Indeed, I became a quite good junior player who could play competitively in a tennis club and even in the Austrian Boy Championship (age bracket 12-14) where I was able to get into the quarterfinals. The tennis league tournament between clubs always included one slot for a junior (up to an age of 18). Unfortunately, I was the only junior of my club interested to play competitively, and this already at an age between 12 and 14. At that early age, I already had to compete with 18-year-old players. I mostly lost such matches, as my competitors were much taller and shot much stronger serves than I was able to do. This was one, but not the only, reason why I increasingly lost interest in tennis; the other was my awakening interest in girls that kept me more and more occupied in the later teenage years. My primary school, then of course gender-separated, was also in the heavily damaged quarter where we lived first in Vienna, and I was fortunate to get a highly motivated and skilled teacher, Mr. Pokorny. I had no problems at all at school; already in kindergarten I had learnt unintentionally everything by listening and looking how my sister in her first class learnt to read and write. Later, I just listened during school lessons and remembered everything, without a need to repeat. At my age of 11, after the first year in a municipal high school, my father was so proud of my school performance to have me switching to an élite gymnasium, the Theresianum that was founded in the 18th century by Empress Maria Theresia for the higher education of kids (of course only boys!) of aristocrats and public officials. At the time, it just re-opened again after WWII with a newly composed team of qualified teachers. It was a private boarding school where about one half of the kids – the interns – lived and slept there and had only occasional permission to visit their families elsewhere in the country. The other half including me – the half-interns – stayed there for the day and went back to the family in the evening, then a highly unusual schooling schedule. Focus was on languages: starting with English at age 10, Latin was added after two years, French after two more years, and finally Russian after one more year. Apparently subconsciously, I decided that three foreign languages should be enough – my schoolmates obviously felt the same –, and took Russian quite lightly. Now I would be most happy if I could read Tolstoy in the original version, but all what has remained is the Cyrillic alphabet and a beautiful poem by Lermontov that we had to learn by heart. We had opportunities to practice all types of sports, including soccer and athletics fields in the huge park, and swimming in an indoor pool. So every early afternoon we rushed out for about two hours, mostly for playing soccer; this was a feeder for my lifelong love for sports and physical exercise in general. However, we also had some 2 or 3 hours of obligatory study time in the late afternoon. We were about 25 boys in our class. While most teachers were real experts in their field, some were less competent in paedagogic terms and even helpless in front of a bunch of merciless juveniles. The same went for the social knit among classmates – there were the usual fluctuating cliques that bullied outsiders. Now, after more than five decades, I still feel ashamed not to have intervened then and would want to apologise to bullied classmates and teachers. Personally, I tried to steer clear of cliques without becoming an outsider, a habit of independence that I have cherished through my whole life. In 1964, at 18, we had our final exam (Matura, Abitur) where I got excellent marks. Our class quickly distributed to all corners of the world, and I met most classmates again only later at reunions after 50 and 55 years. Some proved to have learnt little from life, playing the same clique stereotypes as during their teenage years. Astonishing but probably not so unusual. We had nobody with a medical background in the family. However, since I was some 10 years old, it was absolutely clear to me that I would become a medical doctor. I cannot remember a reason or triggering event, it was a matter of course. My career in (neuro)pathology started with the section of a sparrow who broke its neck by flying against a glass window, and that of a goldfish found dead in an aquarium. I just wanted to know how the inside looked like, and what was the very reason for death. This hunger for knowledge also accompanied my medical studies. I was totally immersed and – although I consider myself a true product of the 1968 generation in attitudes and spirit – in fact did not take much note of, nor participated in, the upheavals and demonstrations that paralysed university life in 1968. I kept this no-commitment tradition in politics for long, with one notable exception: having just graduated as an MD, I participated in a demonstration by doctors for better pay and working conditions. I felt it somehow obligatory to participate, now that I was a doctor myself. A few hundred white-coated people ceremoniously marched down the famous Ringstrasse with banners and slogans, but increasingly my attention was drawn to what happened between demonstrators and onlookers. It was impossible to overlook the strong emotions elicited in surrounding spectators, shouting curses at doctors who were considered privileged over common people and earning too much anyway. It was frightening indeed: a spirit of outright hatred had seized many. With a feeling how easy control might be lost, I decided to never again go to the streets, valid until today. Medical study at the time had a relatively free schedule; you just had to pass some practical exercises and a defined sequence of about 20 rigorous oral examinations, rigorosa. It was up to you how quickly you proceed. An important first step was the practical course in anatomy, with careful dissection of conserved corpses donated for teaching and scientific purposes. A group of 6 to 8 students worked collectively on one corpse during most of the first year, dissecting muscles, nerves and blood vessels in the smelly atmosphere of the phenol-formol fixative. We also had a special brain anatomy course with some dissection work that I found drab and uninspiring. Thank god, this impression did not last. Sitting for long daily hours around the corpses to study and dissect, it was the place to get familiar and make lifelong friends like I did, or, for many, to find partners to marry. The second year included histology, and I soon realised that I had some talent for that. I even gave a crash course to my best friend who initially was unable to recognise anything in microscopic preparations other than coloured spots. Later he became a radiologist – maybe he unconsciously fled into a predominantly black-and-white world. After two and a half year, students switched to the clinical phase, starting with pathologic anatomy, pharmacology and then all major clinical disciplines. I became aware that I had no favourite field at the time. In contrast, many mates were confident where to specialise. At exams, there were only three marks given, excellent, sufficient, and fail, and it was good or bad luck which examiner you got. I can remember almost every single rigorosum. The first one was in medical physics, after the first year. We were a group of no less than 12 examinees, and it was surprising to me that I got a “sufficient” already after a single question that I answered satisfactorily. I did not consider it relevant enough to make an effort to improve the mark. The next exam was in chemistry, with a professor who was probably the most feared examiner of the medical faculty. He was reportedly proud of having a low pass rate, particularly with female students, in my memory the only gender bias that I encountered when studying. My first question was about coenzyme A, a large molecule that I could describe quite well. Then it was me who asked whether I should draw the formula – the professor reacted surprised and agreed. I did it perfectly but was unsure if the professor liked it or not. After quite some more demanding questions, he gave me an “excellent”, my first one in a row until the end, as I could manage to pass all subsequent rigorosa with the best mark. This appeared to be relevant; I had been told that I could become a candidate for a “promotio sub auspiciis praesidentis rei publicae” and be rewarded with employment in a public institution of my choice, at a time when many medical graduates were working as “guest doctors” without salary. Unfortunately it finally turned out that the single lower mark in the initial physics exam did not allow such a distinction. However, I made my way without it. At summer holidays, I had some 3 months to spend until autumn when university life would start again. I had bought a small rubber boat with outboard motor and took unforgettable weeks with a group of friends on the Greek island of Thassos. Days were filled with sunbathing, retsina and ouzo drinking, tavli playing, swimming, snorkelling and fish hunting with a handy harpoon, then still allowed in the Mediterranean. We even vowed to ourselves to live only on what we would be able to hunt. However, fish were mostly lucky, as we said, in fact much too fast for us, and escaped our clumsy attempts. Once we mistook a seagull for a tasty duck and were disgusted to finally have an after-feathering tiny bird to feed four hungry pals. Thus the vow had to be broken soon after arrival, and we raided the next inn to engulf mountains of souvlaki meat with tsatsiki. In addition to these summer delights, I worked as tour guide during other holiday breaks. Usually I had a busload of Austrian tourists, mostly high school teachers, a rather demanding clientele. I was required to execute by myself the local travel organisation with hotels and restaurants, as well as to provide the explanations at sightseeing spots. Of course I had to make detailed preparations and wrote my own manuscript for the whole travel schedule; thus I learnt a lot about countries like Italy, France, Spain, Portugal, Morocco, USA, Mexico and Guatemala. A great personal interest in everything connected with history has emerged from these activities. My favourite trips were those to the absolutely stunning sites of pre-Columbian cultures in Central America, in particular places like the then recently discovered Palenque, Tikal or Teotihuacán, and the unbelievable archaeological museum in Mexico City. Something else that I learnt during the several weeks of staying together with up to 50 people was group dynamics and how to handle critical situations and conflicts that emerged quite regularly. Christmas, Easter and parts of summer holidays were spent that way over subsequent years, and I could earn enough money to buy my own car, first a Fiat Cinquecento and later a Volkswagen beetle, something quite unusual for a student at the time. While it was obvious to me since childhood to have medicine as my lifeblood, the choice of neuropathology was just by chance. My exam in neurology and psychiatry, then still combined and scheduled about half a year before graduation, was decisive for my further career. The professor, a highly respected psychiatrist with a remarkable empathic style, seemed to be pleased by my performance and asked about my future plans; if I were interested in his field, I should meet him again after the end of my study. Of course I was more than delighted, as officially recognised training positions in a given speciality were then almost impossible to get, and I envisaged myself already as renowned psychiatrist. Soberingly, when I came back half a year later with high expectations, he did not appear to remember and emphasized the existence of a long cue of candidates lining up for still unpaid positions. However, I was categorical in that I would never, never work without pay, as I was still living with my parents and wanted desperately to escape from that crowded setting. Hearing that, he asked for my further interests and recommended to make a visit to the Neurological Institute (NI) where my preference should be met best, in his opinion. The NI of the Medical Faculty occupied a full floor in a building shared with histology at Schwarzspanierstrasse, in a block where most pre-clinical institutes were located, in about mid-distance between the main University building at Ringstrasse and the General Hospital (AKH). Since NI was then not involved in teaching to medical students, I had passed by its huge glass-and-white wooden doorway and large lettering of its name many times without entering, when I was on my way to attend histology courses upstairs. None of us students had any idea what was going on behind its doors. Anyway, I made an appointment with its director, Professor Franz Seitelberger, and he welcomed me in his office, with his desk at the very end of an impressively large room. He asked about my interests, and I told him that at the moment I was reading a booklet about biological psychiatry. I read there the description of a (chromatographic, I learnt later) “pink spot” in urine that was claimed as specific for schizophrenia. Wow, this was it! I was absolutely fascinated – an extremely complex psychopathology condensed into a single spot. What could be more exciting to study?! Prof. Seitelberger listened patiently and asked me about many additional private topics like family, hobbies, sports etc. that I considered completely irrelevant. Finally he said, yes, there is a position available. While he mentioned that my pink spot fascination was in neurochemistry, an area also covered by the institute, he emphasised that I would be required to start in neuropathology, a discipline that analyses structural changes in the nervous system during disease, something absolutely basic to all studies of nervous system disorders. Of course I had nothing to object, and we agreed upon my entry to the institute later that autumn. Surely, I remembered to have already liked histology during my study, but wasn’t aware then which chance I would get from the very start: it would become an absolutely perfect fit for my interests and abilities – or did neuropathology choose me? Looking back on my professional life, I cannot imagine something better suited to satisfy a hunger for knowledge and understanding, to experience case histories to evolve like a thriller, to feed any curiosity, to keep your inner fire burning and to help transmitting scientific fascination to others. And the best thing was that it was not only much fun and satisfaction but – very important for me as a young guy who would soon have his own family – you are even paid for it!
Fig. 2. Bust of Heinrich Obersteiner, having its traditional place immediately behind the glass-wooden doorway of the Neurological Institute (NI). My small kids occasionally visited the NI and were greatly impressed by this bust. After asking once to be allowed to tweak the stony cold nose, they did it again every time they visited. After NI’s move to the General University Hospital (AKH) in 1993, the statue was re-located to the Honour Courtyard of the University of Vienna building at Ringstrasse. When I started to work in the NI on Oct. 1st, 1971, nobody could foresee that I would stay there uninterruptedly until my retirement, on the day exactly 40 years later, a straightforward but highly unusual curriculum vitae for a scientific researcher. I realised only later the eminence of the NI as the first multidisciplinary institution of the neurosciences in the world. Founded in 1882 by Heinrich Obersteiner (Fig. 2) and blossoming under Otto Marburg until the collapse of the Medical Faculty by the advent of Nazism, it had become a model for such institutes elsewhere, from Fukuoka in Japan to Montreal, New York and Philadelphia. Absolutely unique was NI’s library that contained an unrivalled treasure of neuroscience books, in particular from the 19th century. It was Franz Seitelberger’s merit to have re-built the NI after WWII, from practically scratch with only a single half-time position, to a nationally and internationally recognised centre of excellence when he became professor emeritus in 1986. At my entry to the NI, it was a composite of several disciplines led by distinguished scientists (Fig. 3). Tumour and autopsy neuropathology was led by Kurt Jellinger; neuromuscular neuropathology by Elfriede Sluga who mainly worked the NI’s own electron microscope; neuropathology of the vegetative nervous system by Gustav Lassmann; neurochemistry by Hans (Hanno) Bernheimer; neurophysiology by Hellmuth Petsche; and neurolinguistics by Karl Gloning. Soon another young aspiring researcher arrived, Hans Lassmann, to establish a lab of experimental neuropathology.
Fig. 3. People working at the NI in the early 1970s. 1st row, sitting from left: Lassmann sen., Petsche, Seitelberger, Jellinger, Gloning; 2nd row: 4th from right, Sluga; 3rd row at left Auff; last row, 2nd from left Budka, 4th Bernheimer. Unnamed persons include the indispensable workforce of technicians and secretaries. Note the distinctive traditional hierarchy, as evident from the arrangement of this photograph, that then imbibed NI’s atmosphere everywhere. In the NI, I was supposed to become Kurt Jellinger’s assistant and, over some 3 years, was given a unique chance to familiarise with neuropathology in my very personal way, by re-examining the huge histopathological collection and compare my fresh impressions with the available written reports. This autodidactic learning style was well in agreement with both my and Kurt’s self-absorbed approach to work. For about half a year, I did not really know how to appropriately re-examine an autopsy case with very large-sized microscopic sections. It took me half a day to microscope such a section, as I mainly used high magnifications and even the oil immersion objective! No wonder that I saw an astonishing new universe of structures of amazing shapes, sizes and colours. After about a couple of weeks of such microscoping, I saw something really bizarre, a rounded body with a strange and multicoloured structure. Consulting not only oil immersion but also textbooks, I could not find anything that resembled this discovery. I got very excited and immediately informed Prof. Seitelberger who, after a shared microscoping session in his office, agreed about the novel character of this strange body. He even suggested to publish it together, and advised me to take microphotographs. Of course I had no idea about microphotographing and admitted that. No problem, he replied and pointed to a small mountain of something hidden under a huge dusty cover in one corner of his room. He would do it himself, as that photomicroscope was the very best in the world. I should come back in about one week. So I asked after one week and weeks thereafter, but he always answered to have been too busy to do it. Then, there was no need anymore to document the strange body: I found out by myself that it was a corpus amylaceum, an extremely common structure produced by astroglia, occasionally looking a bit unusual. As working space was scarce in and between the lab rooms crammed with instruments and equipment, I was given a desk and microscope within the Lecture Hall, a huge room with large windows and old-fashioned seating rows (Fig. 4). Already a postdoc from Japan had arrived, Riki Okeda, a new friend who later became professor of neuropathology at Tokyo Medical and Dental University. Another close friend, Ferenc Garzuly who became Head Neurologist in Szombathely, Hungary, completed our trio there. It was much fun – we had small parties, Riki used to play the violin, and we took everyday a nap after lunchtime snoring in the seat rows. When I recently told Ferenc that I am writing up my memories, he obliged me to mention my first day in the Lecture Hall when I drew onto the chalkboard a cell nucleus to demonstrate a “wonderful” change, but both Ferenc and Riki could not detect anything unusual. Yes, already on my first day I thought to see something special and difficult for others to see. Moreover, according to Ferenc, I must mention to have had a green metal box with some gadgets that made enough noise to prevent both of them from sleeping in the seat rows.
Fig. 4. The Lecture Hall of the NI in 1991 during an informal meeting. Hans Lassmann at far left, the author at right in front, Thomas Berger, the present Director of the Neurological Clinic of the Medical University Vienna, in rows at right, 3rd from front.
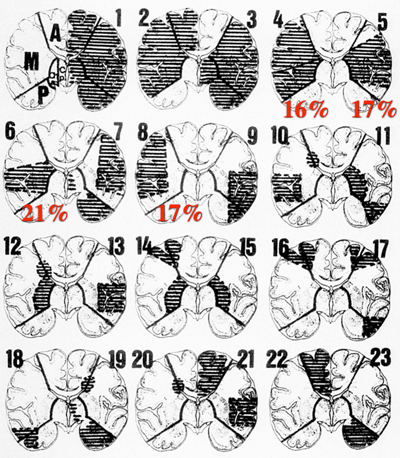
Indeed, it was a great – and by then rather unusual – tradition to always have several postdocs at the NI, in particular from Japan. This started already in the early 20th century when the famous poet Saitṓ Mokichi stayed for 2 years at the NI and wrote some haiku poems there, including so-called tankas that are limited to 31 syllables. One tanka was written about Prof. Obersteiner (translated from German to English by myself): Over several decades, numerous postdocs have been trained in neuropathology in the NI (a long list of names that I can remember is attached at the end of this article). In addition to many Japanese colleagues (who have organised a “Vienna party” whenever I made a visit to Japan), we intentionally kept traditional connections to our neighbouring countries, in particular to those that were behind the iron curtain at the time, such as Hungary, Poland and Yugoslavia. My first student was a bearded guy always wearing black spectacles, Pawel P. Liberski from Łodz, Poland, who was interested to study a rare disease named after Creutzfeldt and Jakob since his first visit in 1979; he became a friend and collaborator during his regular subsequent visits. Two more persons to mention are Takeshi Kurata, professor at the NIH in Tokyo, with whom I published work on virus detection in brain and who also became a friend and regular visitor until today, and Ichiro Akiguchi, professor of neurology at the University of Kyoto, another regular visitor and collaborator on the neuropathological work-up of the community-based VITA study on ageing. He became a friend and invited me several times to stay for up to two weeks in Kyoto, in addition to several trips that I made to all parts of that captivating country. This was to pour oil onto my fire for traditional Japanese lifestyle and culture such as food and onsen baths, as well as Buddhist temples, Shinto shrines and amazing Japanese gardens. After a couple of years, I was allowed to write histopathological reports on neurosurgical biopsies in Kurt’s absence, and autopsy reports on less complicated cases, almost exclusively strokes. I believe there are few neuropathologists in the world (of course with the exception of Charles Miller Fisher) who had the opportunity and gusto to study stroke cases in great detail from the start of their career, and my first book chapter publication was on the neuropathology of cerebrovascular diseases. I am still proud of that early article written in German in the pre-MRI era, now forgotten since decades, because it comprises interesting and original data on the infarct patterns resulting from verified occlusions in the carotid-media system (Fig. 5), demonstrating high interindividual variability and lack of any predictable correlation between site of infarct(s) and site of occlusion [1]. At that time, I was unaware of the importance 1) to publish in English, 2) to publish in a peer-reviewed journal rather than in an obscure multi-author book, and 3) of the relevance to consider bibliometric data such as the impact factor.
Fig. 5. Topographical patterns of brain infarcts in 196 autopsies with verified occlusions in the carotid-media vascular supply. Among the 23 patterns that highlight the eminent individual variability by site and extent of brain infarction, the percentage of the four most frequent patterns (total, subtotal, central and peripheral media infarcts, in sum 71%) are indicated in red. Vascular areas: A = anterior cerebral artery, M = media, P = posterior, ChA = A. choriodea anterior, Cp= A. communicans posterior. Modified from ref. [1]. In that early time, one of my few responsibilities was taking macroscopic photographs during brain cutting sessions, taking place every Wednesday morning (Fig. 6). I made several experiments to optimise that type of documentation: the best background for colour contrast was finally settled as a dark blue, and whole brains and brain slices were arranged on a glass plate some 10 cm above the background cloth, in order not to have any interfering shadows when the illumination was from both sides.
Fig. 6. Brain cutting session with Prof. Seitelberger in the 1980s. Note the numerous fixed brains in glass jars in the back – and the formal ties everybody wore then during work. One more responsibility was to visit the Department of Pathology every early morning, in order to determine which autopsy brains would be interesting and important enough to be fixed for neuropathology. At that time, autopsies still numbered more than 2000 per year, and not every brain could be fixed and examined. I still remember vividly the boss of the autopsy suite, Prof. Kucsko, in the beautiful old building of the Institute of Pathology (now the Institute of Brain Research) where already Carl von Rokitansky had worked. Kucsko was a gaunt chain smoker always with a cigarette butt on his lips during a whole section. He was an extremely experienced pathologist who taught me great respect for the autopsy as golden standard and one of the most difficult tasks in medicine, less with regard to skills but more to generalised knowledge, experience and “feeling”, a talent somewhat difficult to explain by words. Another lesson I learnt from him is the importance of a very detailed macroscopic examination – what you do not see or at least suspect at gross dissection, you have little chance to find by microscopy. Initially he had little consideration for that young guy interested only in the brain. However, once I told him that I found small cancer metastases in the brain when the body section by him had not found anything. Can’t be, he snapped, and went back to the inner organs that fortunately had been fixed and were still available. He called me back in the afternoon to confirm that, indeed, no tumour was found in the body. When I stayed firm with my metastases, he went back again to the fixed organs and finally found, after 3 days of cutting almost every millimetre, a tiny scar carcinoma of the lung. After that I had some reputation with him and was free to express my wishes for neuropathology. This came in handy when Kurt ordered me to freeze fresh brain slices from then relatively many Creutzfeldt-Jakob disease cases autopsied in Vienna. I had to send them on dry ice to D. Carleton Gajdusek at the NIH in Bethesda, for transmission experiments into non-human primates. I did that without any special safety precautions that then were unheard of, and retrospectively I am not sure whether I touched these brains by bare hand or not. I was later very proud to have contributed some part, even when minuscule, to Carleton’s Nobel prize in 1976. Kurt Jellinger left the NI in 1975 for a position of Head of a Department of Neurology in the municipal Lainz Hospital in Vienna where he could do both clinical neurology and neuropathology. Of course, this was a severe blow for the NI, but in particular for me, as suddenly all responsibilities for diagnostic neuropathology were mine. Kurt was the collector type of neuropathologist who always had large case numbers available for his research. During my years with him, the number of neuropathological autopsies was as high as 600 per year, and neurosurgical biopsies numbered around 1000. Only he could handle such a volume alone or with one assistant, and when he left, I – a newcomer with only 3.5 years in business – was almost alone to shoulder such tremendous quantities. I decided quickly to give priority to tumour pathology, and for several years I was unable to keep up with the flow of autopsy cases even when, by necessity, they had to be reduced to a significant extent. To lose Kurt at that time was still more painful to me, as I just had entered into clinical training. Traditionally all MDs of the NI had training in a clinical speciality (to become Facharzt or consultant), usually neurology rather than pathology. Neuropathology became a speciality of its own in Austria only later, a development that I could push forward to a significant extent. To become a specialist in neurology and psychiatry, I started a year of internal medicine in 1974, psychiatry in 1975, and neurology in the following 4 years. It had been agreed beforehand with the directors of the respective clinics that I would do clinical training in the mornings until noon or early afternoon, and then continue my work in the NI where I kept my official position. Under these circumstances, it is not difficult to imagine what workloads I had to face when returning to the NI in the afternoon and working into the night. I soon became unsure whether I could, and should, carry on this double burden at all, a feeling of uneasiness and uncertainty that dominated the second half of my 1970s. Even under these extremely difficult circumstances, I soon realised that research was pre-eminent in importance for the career. As a relative newcomer, I was not sure in which topic I should invest, in preparation for the next step in career building, the habilitation (lectureship, to become Dozent). I had spent most of my year in internal medicine in haemato-oncology, then led by the very amicable Prof. Josef Kühböck, and could witness the successes as well as complications of then modern aggressive and even prophylactic chemotherapy of leukaemia and lymphoma. In parallel, I could collect a small but very interesting and then timely series of brains of patients who unfortunately had died with such complications. Thus I published “The pathology of encephalopathies induced by treatment or prophylaxis of neoplastic lesions of the nervous system”, again as a book chapter that I was proud of but became quickly forgotten; however, this time I wrote in English [2]. Another potential topic that I considered for habilitation was the neuropathological substrate of collagen vascular disease, again a publication that I was very happy with but went practically unnoticed, even in an American journal [3]. Finally, publication of the first description of the adult type of adrenoleukodystrophy (ALD), what is now called adrenomyeloneuropathy (AMN), became a highly cited paper for the first time [4]. In order to be successful, it would be particularly important to introduce to neuropathology, as performed at the NI, new investigations, such as CSF cytology, and techniques such as immunohistochemistry (IHC), in addition to an interesting topic and adequate material to study. I developed CSF cytology with a special sedimentation device, examining CSF samples that I brought to the NI from patients with leukaemia or lymphoma. We counted the number of cells, sedimented them and made a Giemsa stain, later also occasional IHC labellings. For IHC, I started with visualisation of immunoglobulins (Igs), because good antibodies were then available, to be used in direct or indirect immunofluorescence. Astrocytes were usually full of Igs, but soon I realised that no really interesting problem was to be solved with these antibodies. Fortunately, at that time Larry Eng had just purified glial fibrillary acidic protein (GFAP) as astroglia-specific marker and raised antibodies against it, and Lucien Rubinstein – then with Larry in Stanford – had successfully made first immunostainings on brain tumours. Thus the opportunity emerged to introduce IHC for GFAP to the institute, at the start still with immunofluorescence, soon thereafter using Ludwig Sternberger’s elegant peroxidase-antiperoxidase (PAP) technique. Over the next decades, IHC (and to a lesser degree nucleic acid in situ hybridisation, ISH) would dominate most of, if not all, my diagnostic and research work in neuropathology, in particular in neural tumours, infections and neurodegeneration. Of course IHC was also essential for neuromuscular biopsies, but in the old NI they were Elfriede Sluga’s domain, and I entered that field only after she moved, like Kurt earlier, to a position of Head of a Department of Neurology in the municipal Wilhelminen Hospital in Vienna. Much of this work on new techniques must be credited to the indispensable help of our amazing laboratory technicians who patiently and persistently developed perfect (immuno)visualising systems in pioneer experiments: Mrs. Helga Flicker, NI’s all-time good spirit and helping hand who virtually accompanied my whole career in Vienna, Mrs. Irene Leisser who arrived only shortly later, and from the millennial years onwards Mrs. Gerda Ricken. While they kindly agreed to co-author the publication of some of their successes, in fact they should have been on the author ticket of all respective papers. Having said this, any thanks to them would be incomplete without the recognition of work that was accomplished also by other technicians, secretaries and support staff – I was extremely lucky to have such people to work with. Despite all troubles, my early years in neuropathology ended successfully, in 1980 with recognition as clinical specialist (Facharzt) in neurology and psychiatry, a step that also promoted me from assistant to consultant (Oberarzt), and further on in 1982 with my habilitation (lectureship) in neuropathology. The title of my habilitation thesis was “Viral Diseases of the Nervous System” and combined 3 original papers [5-7] on viral antigens in herpes simplex virus (HSV) encephalitis, rabies and subacute sclerosing panencephalitis (SSPE). I was more than happy that the exhausting time of riding two horses at the same time has ended, even when I liked clinical work very much. So it was only later, during my midlife crisis, that I considered to go back to clinical medicine. The turbulent first decade of my professional life coincided with establishment of my own new family. I met Christine at the CSF lab of the Neurological Clinic where she worked as technician, and we married one year later. Philipp was born in 1974, Julia in 1977, Daniel in 1979, and Rafael in 1980. With these kids born in a short period, my wife had stayed at home and it was not that easy for me, as university assistant with a very mediocre salary, to sustain a family of 6. Our financial situation improved somewhat when Prof. Seitelberger allowed me to make forensic expertises that are remunerated additionally. That activity turned out to be demanding but most rewarding intellectually and scientifically, and I have continued it up to this day – something that always has enabled me to keep my fascination for neuropathology alive. With all my obligations, it was very difficult to spend time with the family. I devoted all weekends and holidays to them, but during the week I used to come home from work when most if not all kids were already asleep. We tried to remedy the situation by establishment of a weekly family day when I would come home earlier, play, do storytelling and reading with the kids. Nevertheless, I used to have a guilty conscience about my inability to dedicate enough time that a family with children would deserve. Moreover, we always had dogs that became full family members as well, the wire-haired dachshund Ilko at start, followed by Polski Owcarek Nizinny (Polish Lowland Sheepdog) Betsy and later Hovawart (“farm watcher”) Debbie. Although dogs snip away further bits from your time, they are beautiful and most grateful creatures enriching and rounding up any family; they love you unconditionally, whether you deserve it or not. All my kids grew up to become successful professionals and, more importantly of course, happy, amicable and easygoing personalities to be proud of: Philipp became an established lecturer and researcher in social and cultural anthropology at the University of Vienna and Free University Berlin, specialising in the sociocultural consequences of digital media and technologies, living in a harmonious partnership with Julia, an online media editor. My daughter Julia became an internationally highly respected Egyptologist who repeatedly has performed excavating campaigns in Egypt and Sudan and has won two extremely competitive ERC research grants; she is now Professor of Egyptology at the Ludwig-Maximilian-University Munich and in a partnership with Tanja, a kindergarten supervisor. I admire and envy her, as she is rapidly running up to the number of entries on the internet that I have. Daniel became an expert, art-prize-winning graphic designer and video producer, happily married to Caroline, a hospital physician; they have delightful Ellie and are expecting their second child soon. Rafael succeeded in establishing his own media and marketing company to organise various types of events, from business celebrations to pop concerts, living in partnership with Nathalie, a journalist, and their two gorgeous girls Lori and Noemi. Looking back when getting old, it is most gratifying to see a sequence of generations that carry on the spirit and ideas that you have valued highly during your life, even when my small wish, to have one of my kids enter medicine, has not realised (but I still have such hopes for my fifth child, Natalia). The difficult family years had one casualty, as it turned out only later. My marriage broke apart, fortunately only when all kids had already left our home. Certainly a divorce, and mine was a bitter and battled one, is a sad event in any life. However, to quote Paul Watzlawik, there is nothing bad in life that doesn’t have something good as well: my longstanding guilty conscience about the inability to dedicate enough time to the family fell apart quickly, and I suddenly felt completely free, a feeling of happiness and contentment that I had missed since decades. Of course it is a very selfish thing to be back to independence, but my advice to everybody is to listen to one’s very gut feelings how you really sense your being. I discussed the situation that I went through with friends, and some of them had similar constellations; a couple of them did the same as I – and these made identical experiences. In the following years I was free to work as I wanted, to travel around as I wanted, and to have no private commitments at all. The most important matter, however, was continuation of my good relation with all children despite the divorce. Going international and something other than work Totally focused on work and a growing family, I had neither time nor interest for the many distractions young people had at the time. A somewhat more relaxed schedule was possible when I went to scientific meetings and congresses outside of Vienna. From early on, I tried to attend International Congresses of Neuropathology (ICNs), the biggest event in our field. My first ICN was in 1974 in Budapest, and the technique that dominated most investigations was electron microscopy, with “virus-like structures” almost everywhere. Brain tumour pathology, for the very last time, had retained a strong influence by Spanish and Latin American researchers using sophisticated gold and silver techniques as basis for classification – we dubbed a symposium chaired by the famous Professor Moises Polak in Budapest as “metal mining” meeting. Within the few following years, the centre of gravity shifted to the Anglo-American tumour tradition, mostly represented by the landmark book editions by Dorothy S. Russel and Lucien J. Rubinstein, then the bible and only comparable in impact to the present WHO Classification of Tumours of the Central Nervous System. When the ICN in 1982 was held in Vienna, I was charged with organising a tumour slide seminar together with Lucien. It was an unbelievable luck and privilege to meet, discuss and work with such a giant. I visited him in Charlottesville, VA, well before the ICN in order to select interesting candidate cases to present. What impressed me most was his memory with the incredibly huge collection of ”similar” cases that he had at his fingertips – whatever you showed and asked, he immediately answered convincingly with demonstration at the microscope of a similar case. By the way, he was equally impressive as an impeccable British gentleman (although originally from Belgium), almost seeming misplaced in the US (he could have been the topic of Sting’s song ”Englishman in New York”, in particular the quote “If manners maketh man, as someone said, He's that hero of the day”), as a true polyhistor with amazing knowledge of art (he decorated his home with stunning huge tapestries by Jean Lurçat), and as husband to a most charming and warm-hearted wife, Mary M. Herman, also a neuropathologist and his closest collaborator, with particular EM expertise. In addition to ICNs that are only held every 3 or 4 years, I regularly attended annual meetings in Austria’s great neighbour, Germany, i.e. those of the German Society of Neuropathology and Neuroanatomy. In addition to a much broader scientific scope than what we had in small Austria, those meetings were nice social events to meet new and old friends, in a relaxed atmosphere that sometimes culminated in rather hilarious sessions, unexpectedly in business sessions of society members. I remember some colleagues with unbelievable humour, such as an extremely witty guy from Frankfurt, Prof. Thomas. Everybody was already holding back laughter when he started to speak and made bizarre suggestions. One of the early German meetings that I attended, in 1979, was held together with the Polish Society of Neuropathology in Cracow. I went there by car, then quite a trip across countries behind the iron curtain, and highways were still non-existing on that route. I went there also to have a glimpse of Cieszyn / Těšín / Teschen from where my grandfather had migrated to Vienna. I arrived there late in the evening, and the impression was appalling, as the town appeared completely dark, depopulated and dilapidated; in my thoughts I congratulated my grandfather to have escaped from there. For fairness: when I came back 40 years later, it was a very nice and well-maintained Central European town with a huge historical main square, deserving a visit. The meeting in Cracow was nice, the city very beautiful and full of history, but I looked also elsewhere and soon found out that Auschwitz was close. I thought that it would be obvious, even obligatory, to make a visit to such a historical site nearby. Therefore I asked at the German society members’ business meeting about the tour that certainly would be organised there and whether a place was free for me to join. Totally naïve as a youngster who was spared from the horrors of the Nazi period by the blessing of late birth, I did not expect that my question would raise any nerve, but it did. There was icy silence, and nobody wanted, dared, or was interested, to answer. My god, I thought, this was then at least 34 years ago. Good lesson for my naïvety. It was only later that I learnt of the involvement of some Austrian and German neuropathologists in Nazi atrocities, but also of the admirable efforts by some, in particular by Prof. Jürgen Peiffer from Tübingen, to elucidate and document the disastrous deviation of our discipline during that period. Twenty years later, after I became director of the NI, I had to re-visit and clean up such involvement in our own backyard. To some degree, the visit to Auschwitz changed my life. The main camp, Auschwitz I, had been restored as a museum that was well maintained and diligently documented, with all the horrors of gallows, execution walls, mountains of hairs, spectacles or children’s shoes, all difficult or impossible to stomach. However, the extermination camp proper, Auschwitz II – Birkenau, was different; it was kept as it was, without any restoration, additions or changes, giving it a surreal atmosphere of the still present, villainous evil as well as persistent agony. I spent the whole day there, wandering around completely distraught, aimlessly and disoriented, sometimes hallucinating victims’ whispers. It took me a few days to get over this experience, and I decided for myself to contribute my very own, very personal, however small, part to have that never to happen again. Back to Vienna, I identified Amnesty International (AI) as perfect fit for my abilities and intentions, and founded the first AI Medical Doctors’ group there. AI’s remit is to fight human rights abuses, torture and death penalty everywhere in the world. Then it was still cold war – the fight against lawbreakers and offending countries was three-tiered, politically balanced between the West, countries behind the Iron Curtain, and those in the developing world. Medical doctors had a definite role in that fight. As examples, our group documented objective signs of torture in victims who were lucky to have escaped to Austria during and after the Iranian revolution or from Latin American dictatorships. I also participated in missions that investigated and reported on conditions of prisons in countries accused of abuses in jail, another disturbing personal experience. Since AI does not provide direct treatment to affected people, Siroos Mirzaei, a radiologist and amicable friend with Iranian roots, and I decided later to proceed with an organisation called Hemayat (meaning help or protection in Arab and Persian) that was to provide free psychological and physical treatment for victims of torture in Vienna. The Balkans war of the 1990s created many, often too many, victims in need of help. In this year, Hemayat celebrated its 25th anniversary – and is still necessary to exist, maybe now more than ever. By the first half of the 1980s, I had investigated the regional and cellular tropism in a range of viral infections involving the nervous system, but nobody had previously assumed that this knowledge would become very helpful when, since 1981 in the USA and then in Europe, a new disease appeared apparently out of the blue, acquired immune deficiency syndrome (AIDS). In Austria, we had our first autopsies from early 1983, and we were well aware that appropriate safety measures had to be applied, although only later that year Luc Montagnier (with Françoise Barré-Sinoussi, also sharing with her the Nobel Prize in 2008) isolated the culprit as lymphadenopathy-associated virus (LAV), or HTLV-III as Bob Gallo called it, or human immunodeficiency virus (HIV) since 1986. I could meet and listen to these two eminent researchers, both of whom gave the immediate impression to be characters as different and irreconcilable as possible to imagine, maybe one of the reasons for their bitter fight for recognition as HIV discoverers and exploiters. When I had examined a small series of AIDS brains, I realised there was something going on in addition to the by then well known opportunistic infections, an inflammatory process with multinucleated haematogenous cells as hallmark. I published that in 1986 [8], after having described with Paul Kleihues from Zurich another characteristic type of pathology, a progressive diffuse leukoencephalopathy [9]. In those years, I was busy with presenting my HIV data at lectures and meetings. After such a meeting in Germany, a well-known professor took me aside and asked: “Well, I also have a series of HIV brains but have never found the multinucleated cells you describe!”. I replied by suggesting to show me slides of whatever case he wanted to discuss, and it was perfect luck for me to find almost immediately these cells in his own slides. “Oh, they look like this, I didn’t expect that!” was his reaction. Yes indeed, these cells may look somewhat strange occasionally and differ from other types of multinucleated cells. One lesson that I took from that and similar situations was my absolute belief in the old wisdom that there is a lot to see when you look, and in old-fashioned, analogue microscoping for training, when one can play around with focus over several planes, something that is difficult to impossible to experience with simple pictures or even more advanced digital slide processing. So up to today, I refuse to give diagnoses just on cabled images. Exactly at that time I met Gianriccardo Trabattoni, an extremely big-hearted neurologist from Parma, Italy, having striking similarities in physiognomy and humour with Woody Allen. He asked whether I would be interested to study autopsy brains from the AIDS epidemic in Italy. An enormous tragedy was then occurring in Milan, with many deaths every day. Now this sad history repeats itself there, with the difference that SARS-CoV-2 kills preferentially old people, whereas HIV killed indiscriminately, including many youngsters. Yes, no question, I was interested to study those brains, and Gianriccardo spent subsequent weeks in smuggling caseloads of formol-fixed brains in jam glass jars by rail across the Brenner frontier from Italy into Austria. At that time, there were still border controls, and I wondered what would happen if he would have had his luggage controlled – I had nightmares of press headlines roaring “Band of brain smugglers arrested” or, still worse, “Scientists uncovered as graverobbers”. Almost immediately we had several dozens of brains, and in 1987 we published our combined neuropathological experience from 100 AIDS autopsies, including most beautiful EM photographs of HIV virions provided by Silvia Cristina, a very gifted pathologist [10]. The next step was visualisation of HIV products in the brain, as I had done previously with other viral infections, and detailed determination of cell tropism in the brain [11]. As already suggested in my work on the multinucleated giant cells of HIV encephalitis, productive infection was seen exclusively in microglia and macrophages, a new paradigm of infection and inflammation in the brain, with neural elements proper not participating in virus replication and production. However, neurons are secondarily affected: in collaboration with Prof. Haug’s neuroanatomy group in Lübeck, we demonstrated by morphometry neuronal loss in AIDS brains [12], in addition to HIV encephalitis and leukoencephalopathy another substrate of HIV-associated neurological disorders (HAND). My career in neuropathology was successfully under way when, almost exactly at midterm of my period in the NI and at the age of 44, the confidence in my future was shattered. In 1990, I had two invitations for meetings in India, one to speak at the World Neurology Congress in New Delhi on HIV and the nervous system, and another to contribute to a specialised satellite symposium on SSPE at the famous Christian Medical College in Vellore, a more than 100 years old foundation in a city in the South, originally for women only, with an affiliated hospital, by now one of the premier such institutions in India. Whenever participating at scientific meetings, I always try to squeeze off a few days for my own sightseeing, on and off the beaten track, in particular when it was the first time for me in that area. Then it was my first time in India, and I was shocked to verify myself the amount of poverty and suffering on the streets, with people lying and dying on crammed sidewalks in the North. To some contrast, the South seemed better off, with less pressure by sheer numbers of people and a friendly tropical climate. The meeting in Vellore was organised by Dr. Jacob John, already then an eminent virologist who fortunately makes his expert opinion still heard now on CoVID-19. I was much impressed, but still more when he took us foreign participants to the hospital ward to meet patients with infections in India. As neuropathologists, usually we do not see individual fates and histories behind our fascinating stains and slides; so first-hand experience by meeting patients with diseases of our study topics is a completely different dimension. They had several boys with SSPE in the ward, for most of us now an interesting but extremely rare if not exotic condition; however, I would wish that anti-vaccinationists could see the devastating and deadly disease that is preventable by measles vaccination. Other interesting cases included what I discussed with Dr. John as Tropical Spastic Paraparesis, then a new retrovirus-mediated disorder, tuberculoma and many unclear conditions. I became speechless seeing all that. Apparently this experience well coincided with what was emotionally my midlife crisis – I spent the following nights and days seriously considering to drop out of my safe harbour of academic work, career and family life and start again from scratch with clinical work in a place like Southern India, where your personal contribution to alleviate sufferings could really make a difference. I turned pros and cons in my mind, realising that the youngest of my kids was already 10 years old, so it would be not that damaging for their upbringing if I would leave, whereas their economic future might become uncertain. The longer I pondered these considerations, the paler the memory of South India became, and finally these ideas faded away. Apparently I had no guts for a complete new start, and it was much more convenient to follow in the prepared footsteps of one’s comfortable life. Do I regret it? I am not sure, even now when I am very happy with my life track, and probably any present thoughts on what-would-have-been are more coquetry than deep-hearted wishes. National and international neuropathology The 1990s were an important period for the old NI. After more than 100 years, its facilities moved in 1993 from the old building at Schwarspanierstrasse to the newly built university hospital, the New Allgemeines Krankenhaus (AKH) where NI was renamed as Clinical Institute of Neurology (KIN) and located in the ground floor at the southeast corner of the enormous main building. I had been involved in planning for the new location since more than a decade and was proud to have achieved a consented plan offering unique facilities for the future. The move itself was one of my worst experiences, and I commuted for weeks from the old to the new building. KIN was provided in the new quarters with generous space and top-class laboratories featuring most modern equipments for neuropathology (including an own EM and tissue culture), neurochemistry and molecular neurobiology. What was still missing I could manage to have added in later years, such as a dedicated prion BSL-3** lab, laser scanning and confocal microscopes and laser microdissecting device. The downside was that the other multidisciplinary but non-clinical parts of the old NI were not transferred as well, but moved to a brand-new Institute of Brain Research in the completely refurbished building of the former Institute of Pathology, with Hans Lassmann appointed as Professor of Neuroimmunology and first Director. For the clinically working parts of the old NI, now the KIN, the environment of a modern university hospital turned out to be most beneficial, not only for diagnostic service, but also for research and teaching. After I became full professor and Director of KIN, I followed the research output by publications year by year, and from very modest scores in the early 1990s, a regular increase of cumulative impact factors per year became evident, surpassing 100 in the last years that I served as director until 2011. The move to the AKH was also favourable for teaching. Although NI had been involved in some practical courses to undergraduates, KIN became increasingly involved with teaching lessons for Clinics of Neurology, Psychiatry and the Institute of Pathology. Usually selected topics of the neuropathological spectrum of diseases of the nervous system were lectured, but I always tried to include some of my very own concerns for future MDs. One general was functional neuroanatomy that I found rather underrepresented in students’ knowledge and understanding, and another specific was brain trauma, in particular by voluntary activities such as boxing, with the aim to inflict – or at least tolerate – brain damage to others, an issue that should prevent its performance as sport. Such new success did not happen without shadows. When describing above my early experience at a German congress in Poland with regard to a visit to Auschwitz, I mentioned also the need to clean up the institute’s backyard. It was only very late, around the turn of the millennium, that efforts were made by the University of Vienna and its Medical Faculty (from 2004 the new Medical University of Vienna) to finally clarify, document and purge any remains of the Nazi past. For the institute, it turned out that the neuropathological archive contained brain samples, mostly processed histological slides and blocks, of “handicapped” persons in mental institutions, mostly kids, who had been murdered within the Nazi “Euthanasia” Program. In Vienna, the psychiatric institution “Am Spiegelgrund” was the place where these killings occurred, and brains of victims were collected and neuropathologically examined – later unbelievably supported by public funds – by Heinrich Gross who had also a role in the killings. For further research, some samples were later brought by Gross to the NI, and much later I had to identify and de-archive such specimens that were then ceremoniously laid to rest in a dedicated memorial tomb at the Vienna Central Cemetery. Additional data by Jürgen Peiffer from Tübingen revealed that brains with a peculiar neuropathological disease from three brothers, murdered in the Landesanstalt Görden in Brandenburg, Germany, were first described by Franz Seitelberger as connatal type of Pelizaeus-Merzbacher disease (known today to be due to missense mutations in the PLP1 gene) in his thesis for habilitation. The samples had originally been archived in the Max-Planck-Institute for Brain Research in Gießen, Germany, headed by Julius Hallervorden who had been heavily involved in the neuropathological work-up of brains of victims of Nazi “Euthanasia”. Seitelberger had spent a postdoc stint in Gießen and brought these samples to Vienna and the NI. Again, I identified these samples in the archive and sent them to Hamburg where they were ceremoniously laid to final rest. As a small discipline, neuropathology relies very much on international contacts, interdisciplinary discussions, connections with colleagues and friends, and communication at meetings. Having realised this soon, I have fostered such contacts by personal visits, invitations and correspondence. In addition to diagnostic matters, it was research that was, and still is, most in need of international networking. An overlapping field encompassing both diagnostic work and research like neuropathology has classification of disease as a necessary but also possibly arbitrary component of biomedical science and practice. Nowhere this was more evident than in the field of pathology of tumours of the nervous system that has been based on histogenetic concepts since long but clouded by complexity over generations. During medical studies, most of my colleagues just skipped the several pages of brain tumour types in our learning documents, as the classification given there was considered counterintuitive, intricate, confusing in places and simply too cumbersome to absorb. This fact has been recognised by the WHO that reacted by publication of the Blue Book series on tumour pathology. The 1st Blue Book on “Histological Typing of Tumours of the Central Nervous System” was edited in 1979 by Klaus Joachim Zülch, an eminent neurologist-neuropathologist in Cologne-Merheim, and appeared, at least to outsiders, as compromise between Zülch’s classical German tradition of neuropathology and the Anglo-American school represented by Lucien Rubinstein. As example, it included the monstrocellular sarcoma, one of Zülch’s dearest entities as sarcoma because of a distinctive network of reticulin fibres, as well as the monstrocellular glioblastoma championed by Rubinstein because of GFAP immunopositivity, both the very same tumour type. Thus most of the complexity remained. As I had to diagnose large numbers of neurosurgical biopsies, I applied my immunohistochemical expertise from my studies on viruses to CNS tumours and always tried to keep abreast of current trends. Much credit is due to Paul Kleihues, then Professor of Neuropathology in Zurich, to make an effort to renew brain tumour classification in a modern system that took account of molecular and genetic characteristics and did not only rely on morphology. A meeting was convened in Zurich in 1990, with 26 distinguished experts in neurooncological pathology, almost all male, including me, and only two renowned female researchers, Lucy B. Rorke and Ana Lia Taratuto. One giant was notably missing – Lucien Rubinstein had died from brain haemorrhage briefly before. The result of intense deliberations – to include new entities, in particular the concept of primitive neuroectodermal tumour (PNET), and delete obsolete ones like the monstrocellular sarcoma – was finally published in 1993 as 2nd edition of the Blue book. The 3rd edition in 1997 and its update of 2000 followed meetings in Lyon in 1997 and 1999, were re-titled as “Pathology and Genetics of Tumours of the Nervous System”, had expansion on genetics and were published by the International Society of Neuropathology (ISN) together with the International Agency for Research on Cancer (IARC) that was then directed by Paul Kleihues. The 4th edition in 2007 and its revision in 2016 returned to the title “WHO Classification of Tumours of the Central Nervous System” of the old Blue Books. All these editions proved to be an indispensable tool for neuropathologists not only in their daily diagnostic work, but also in use of a common language with clinical colleagues and basic researchers. I have contributed to all editions and was mostly happy with the outcome, with one exception: I remained sceptical about the scientific rigour and value of the WHO grading system that applied four uniform prognostic categories across all types of tumours and was carried on unchanged since the very start in 1979. We had heated discussions at all meetings on that issue, but Paul was a passionate and dominant defender of WHO grading. Moreover, he was clever enough to put discussions on this topic to the very end of the agenda – usually there was not enough time left for debates in depth. Based on my experience with tumour neuropathology, I realised the importance of working with established national and international bodies with regard to diagnostic matters, research and fostering of the discipline. Thus I have served for several periods as President of the Austrian Society of Neuropathology. In Europe, the supranational European Confederation of Neuropathological Societies (Euro-CNS) is the contact for professional matters, and I became president in the early 2000s. The International Society of Neuropathology (ISN) is the global representative of our discipline, and I have served as national Councillor, as Vice-President and finally as President from 2010 to 2014. Many scientists have disgust for such officer honours and “committology” in general, as they feel it much more rewarding to spend time in the lab than in discussions at formal administrative meetings. Indeed, such meetings may produce little more than hot air, but my experience tells it depends on you – yes, on you in whatever function you attend – how productive or not your participation will be. Moreover, don't forget: If you don’t commit yourself to meetings, there is always a possibility of non-transparent agreements negotiated in back rooms by parties attempting to over-rule others, something nobody wishes (or claims so…). In the early 1990s, I realised that the type of HIV neuropathological studies, as I had done for almost a decade, was unlikely to contribute much novelty to our future understanding. So where to look next? In the field of infections, a new paradigm was emerging that overlapped with neurodegeneration – something called prion, an infectious proteinaceous particle, a name coined by the later Nobel laureate Stan Prusiner for agents causing transmissible spongiform encephalopathies, then still hotly debated and regarded by many as viruses or virus-like agents. In Austria, we had a disease dubbed as “Austrian Kuru” by Franz Seitelberger who studied the neuropathology of several cases of a family condition first described by Josef Gerstmann, Ernst Sträussler and I. Scheinker in 1936, now usually abbreviated as GSS. Scheinker's first name initial would mean Isaac, as I found out, a name not appropriate in Germany under Nazi rule. Featuring prominent amyloid plaques, the pathology indeed resembled that of Kuru, the New Papuan disease that D. Carleton Gajdusek transmitted to chimpanzees, like he did later also with Creutzfeldt-Jakob disease (CJD). Again, I stepped into that research field more or less by chance – or by another good luck? Fortunately, I had some reputation with the then professor of neurology in the university hospital Vienna, Herbert Reisner. He sometimes called for my opinion when he suspected strange and rare clinical cases. As example, I could diagnose the first clinical case of progressive supranuclear palsy, a disease then practically unheard of by clinicians in Vienna. Once he even took me as company when he got a call from the Veterinary University to consult on a horse with a strange gait disorder. We came to the stable holding the horse, to have a look how the animal moved. The horse was there, but Prof. Reisner not – he had immediately hidden behind the door and told me to examine the horse in his absence. I learnt later that, possibly as sequel of war trauma, he hated horses and was terrified by them. The horse suffered from what veterinarians called a “wobbler”, a yet rather unspecified ataxic condition, and I had to decide myself what to recommend. Guess what my, a neuropathologist’s, recommendation was? Euthanasia and neuropathological examination to get a final diagnosis, something that turned out not to be feasible because of severe squeezing artefactual damage of the thick equine spinal cord when the mortuary assistants pulled it out like a rope. In 1990 Prof. Reisner asked me for an opinion on a rare case that some considered as CJD. The middle-aged lady had indeed symptoms and signs indicative of CJD, but additional spinal long tract signs were unusual, and I had a yet unspecified feeling of something very special. Normally, I never think of it, but here I looked for the maiden name of the patient. Bingo! It was “H”, the name of a family that I knew very well from earlier studies of important cases in the archive of the NI – I had discovered a new case of the original Austrian GSS kindred! It had been completely lost to follow up since some 30 years, as family members were dissatisfied by their experience with medical doctors who were unable to help them; some even told them to belong to a “syphilitic family”, since spinal long tract signs are characteristic of Tabes dorsalis. In the small villages south of Vienna where most of the family lived, this was not something to like to hear or speak about. Anyway, the re-discovery enabled us to complete the full pedigree to 221 members in nine generations from the late 18th century onward, with at least 20 patients suffering from definite GSS, our last proposita presenting a switch from classical GSS to a CJD-like phenotype [13]. We tried over the following years to find out why and how a disease with the very same genetic aberration in the same family was able to change the phenotype, but this has remained elusive. Anyway, it was reassuring to find the salient P102L mutation in the prion protein gene PRNP also in the original GSS family, in collaboration with Hans Kretzschmar from Munich [14]. From 1994 onwards, initially well before the advent of variant CJD (vCJD), I succeeded in coordinating a series of large European networking projects funded by the European Commission (EC). The aim was to establish and apply diagnostic criteria in the neuropathological assessment of human prion disease, to determine their clinicopathological phenotypic spectrum and work on specific research issue related to tissue pathology. These projects perfectly complemented other EC projects coordinated by Bob Will from Edinburgh on clinical surveillance of human prion diseases. It was a pleasure and privilege to collaborate with Bob for many years on these challenging issues, and to make many good friends in the prion surveillance system, including Heino Diringer, Paul Brown, James Ironside, Maurizio Pocchiari, Fabrizio Tagliavini, Inga Zerr, Pawel Liberski…. The scientific collaboration within such networks was strengthened by meetings at regular intervals; my own EC projects had their meetings usually in the small town of Baden near Vienna, a historical spa type of place popular already in the Austro-Hungarian Empire. The huge bonus of these meetings were the limited number of participants (usually between 50 and 100), lectures on timely and emerging prion issues by top researchers followed by enough time for detailed discussions, and half a day reserved for socialising, walking and hiking. Following these simple rules, these meetings have become almost legendary in retrospect – whenever I meet people who had attended, it becomes a nostalgic exchange of memories. Baden is amidst a wonderful, wine-growing landscape at the very Eastern end of the Alps, where pleasant hills of the Viennese Woods come down to the Pannonian planes, so hiking there was always a most enjoyable activity – and sometimes a true escapade to remember. As the Baden area was not too familiar to me and we had to keep our time schedule, I wanted somebody to guide us on our hiking tours. I have a friend who lives in the area, Erich, a retired high school teacher who described himself as knowing every rock in the vicinity and was enthusiastic to take over the organisation and guidance of our hike. It was an unusually hot day in early June, and the first part of the track was steeply uphill for about 45 minutes. Erich calmed down early wishes for a break by promising a mountain lodge on top. When we arrived, thirst was significant, as was disappointment: the lodge was closed for restauration. No problem for Erich: as he knew all hidden details of that part of the forest, he promised to get us to a spring with wonderful fresh water. Of course, in order to get there, we had to leave the marked trail and step into the dark forest. I had advised everybody in the 40-plus-numbering group of hikers to wear strong walking shoes, but some ladies apparently misunderstood that as invitation to test the most modern and glitzy slippers then available. As to expect, it was not that easy for such a poorly equipped party to walk across thickly covered forest floor. Finally arriving exhausted at the spring, another disappointment and still more reason for thirst: the spring had dried up, and Erich had some trouble to explain why he had not been aware of an unusually prolonged dry period in the immediate past. Feelings of despair were palpable, and I decided in a revolutionary mood to take command. I phoned our bus driver, ordered him to buy a supply of boxes with hectolitres of water bottles and come to the nearest parking spot where a bus could go. It was still some more 45 minutes to walk there, but fortunately downhill below shady trees, so a full rebellion by the party could be avoided by repeated announcements how near the bus parking already was. When we arrived at the bus, exsiccated and with ragged clothes, everybody offered a fortune for a drop of water. I threw away my chances to get such a fortune, like always, and gave the water for free. Finally, whatever worries people had, they disappeared suddenly and were replaced by everlasting memories of an exciting adventure. The work on human prion diseases coincided with emergence since the late 1980s of a new animal disease, bovine spongiform encephalopathy (BSE), aka mad cow disease. Hundreds of thousands of bovines were affected, had to be slaughtered and disposed of in the UK. This economic disaster accompanied loss of public confidence in politics, a phenomenon that spilled over also to continental Europe where BSE became a problem only delayed, from around 2000. In 1996, the high water mark broke when UK government officials had to concede that BSE had transmitted to humans in form of another new disease, variant CJD (vCJD). Proof for that, of course, came by neuropathology: James Ironside in Bob Will’s group demonstrated characteristics of a new prion neuropathology. Immediately, some hysterical press releases forecasted an armageddon of millions of victims, and feverishly reactions and solutions were deliberated, in the UK as well as in the European Union (EU). This was the hour of experts – however, at the time few were there, as prion diseases had been the domain of a small group of basic researchers in biochemistry, of veterinarians working on scrapie, the prototype prion disease in small ruminants, and of medical specialists in epidemiology, neurology and – you are right again in guessing – neuropathology. Surveillance for human prion diseases became quickly established throughout Europe and needed neurologists, laboratory specialists and neuropathologists. In Austria, the Austrian Reference Centre for Human Prion Diseases (ÖRPE) was formally established at the NI and funded by the Ministry of Health. ÖRPE served as national focal point as well as representative for international contacts in the quickly enlarging prion arena. I was head of ÖRPE from 1996 until 2012 when I left to work in Zurich. At the time of the BSE/vCJD meltdown, the top scientific advisory body in the EU was the Scientific Steering Committee (SSC) that quickly established its own prion advisory panel, the TSE/BSE Ad Hoc Group with about 20 members with experience in all aspects of these diseases. I had the privilege to be chosen as member, and from 1997 we had meetings in Brussels every month or even more often. For preparation of these meetings we were sent exhaustive documents, sometimes numbering hundreds of pages. The pressure was considerable, but the panel was highly successful to recommend a series of comprehensive measures to mitigate the risk, most notably with regard to the safety of animal-derived products, identification for destruction of specified risk materials in the food and feed chains, quantification of the residual BSE risk in food, and country-wise evaluation of the geographical BSE risk according to a standardised set of parameters [15]. It was a most interesting experience, as everything had not only public health and economic, but also political implications. In contrast to some members of the SSC, the TSE/BSE Ad Hoc Group appeared to me more reluctant and cautious, and in the group I worked most closely with Dominique Dormont and Hans Kretzschmar. They were not only wonderful scientists and friends, but had the very same cautious approach to a situation with many unknowns. We even insisted on a minority report when we disagreed with the SSC on a pivotal issue. Now, years after they have died, I still miss them. When it became clear in 2000 that BSE was present in continental Europe, we also had in Austria our first BSE cases that put the government into a panic-stricken work mode. Restaurants in Vienna were particularly affected by the BSE crisis, as boiled beef from Tafelspitz, a peculiar meat cut, is a traditional delicacy that, as the saying goes, was never missing at Francis Joseph’s imperial table (* Note to gourmets: my personal preference is not the famous Tafelspitz that I find too dry, but some cuts with slightly fatter composition like Schulterscherzel or really fat Beinfleisch, or Kruspelspitz with a small cartilage. This must be served within a beef broth garnished with slices of bone marrow tasting like paradise on toasted dark bread). For a few weeks, I was interviewed many times by TV and radio, and in the midst of this turmoil I got a phone call from a governmental secretary to invite me to a “beef dinner” with the Austrian Federal Chancellor, the head of government, the Federal Minster of Agriculture – and me. Although having never been a member of a political party or movement, I smelled that the aim was to stage a televised public event at which the safety of Austrian beef should be verified beyond doubts by shared politico-scientific consumption of Tafelspitz. I respectfully declined the invitation and explained that I loved boiled beef but that I was in science and medicine but not in political activism. Retrospectively, some might argue that I missed a chance to climb up the career ladder, but I was happy with what I got – and then indeed did not rise higher. After 2003, scientific advice and risk assessments were continued by the newly established European Food Safety Authority (EFSA); prion-related issues were handled by its Biohazard Panel. Again, I became a member, later its vice-chairman, until 2012. Monthly two-day meetings were held, at first in Brussels and, after completion of the new EFSA headquarters, in Parma, Italy. Numerous opinions on various aspects of food safety were the outcome of our work there. With regard to BSE, vCJD and other human prion diseases, it became clear that scientific advice on risk mitigation has resulted in almost complete disappearance of classical BSE, a real success story, whereas other prion problems persist [16]. During the long years with EFSA the beautiful and historical city of Parma became dear to me, as did the colleagues in the panel – it was a constructive and open atmosphere that I enjoyed very much. As Parma is the very food capital of Italy, we had of course splendid dinners there. My favourite was il bollito misto de Parma, a famous dish with meats from cheek, tongue, tail, belly and head, mostly beef, some stuffed but all just boiled, sounding like components of Scottish haggis, but reminding me more of the typical Viennese Tafelspitz. As the Habsburgs used to export princesses as monarchic wives all over Europe, Maria Luisa, the daughter of Austrian emperor Francis II, who had been Napoleon’s second wife and thus Empress of France, was later made duchess of Parma. Maria Luisa had great impact on Parma, and there are still Austrian souvenirs in Parma, with the bollito probably as one of the most prominent. Upon request, I can advise on the best ristorante for bollito. How do you measure success in science? Depends. As always, money counts also in research, no question. Thus it is essential, already early in a career, to acquire research funds from whatever source possible, something that needs to be trained, as amounts of funds collected for research, patents etc. have become one hard currency of measuring success in science. The other is publications; there are now bibliometric parameters that determine work, career and even the very existence of scientists. This can be considered good or bad, but it definitely is not all what counts. In the present world of multi-authorships, sometimes diluted up to 100 co-authors or more, I am proud to have been one of the very few who wrote many articles as single author, without the safety net of helping hands. Of course, this has become different nowadays – present science by necessity has become teamwork, even a world-spanning network. Another aspect is the range of research, whether it is narrow and limited to a single problem or wider. For an academic career – and I have witnessed that from sitting on a plethora of search committees for academic positions – it is important to prove both depth and breadth in research. As a now almost extinct species in this regard, I am also proud of having published in virtually every field of the discipline, from developmental neuropathology over metabolic and toxic, inflammatory, infectious and vascular diseases to neurodegeneration, tumours and neuromuscular disorders. Many papers have been highly cited, and I have achieved a high Hirsch index – the beauty with that, in my view, is its steady growing, even when you publish little at present, as I do. However, what is really important is to have made new contributions to the general body of knowledge, such as I did with first observations or conceptual outlines, as our report in collaboration with Kenji Kosaka about a case series with neocortical Lewy bodies characterising a new disease, now called Lewy body dementia [17]; or neuropathological diagnostic criteria for CJD [18], neuropathological features [19] and other aspects of prion diseases [13, 14 and many others] including the subcellular localisation of disease-associated prion protein [20] and characterisation of a new disease in wild-type animals by synthetic prions [21]; the neuropathology of HIV infection [10, 22 and many others], viral products in tick-borne encephalitis [23]; GFAP in oligodendrogliomas [24], the clinical relevance of meningioma subtypes [25]; a new glial globular tauopathy [26], nigral burden of α–synuclein as a correlate of striatal dopamine deficit in Parkinson’s disease [27], morphological evidence of α–synuclein propagation in the human brain [28], the basis of biomarker diagnostics in neurodegeneration [29], the frequent mixture of neurodegenerative pathologies in the aging community [30], and transmission of Aβ by dural grafting [31]. After transfer of the old NI into the AKH, we established several clinical routine processes to support our daily work in an expanded environment, such as weekly conferences with the whole staff, research reporting meetings and time-fixed daily microscoping sessions around a multi-ocular device that was able to accommodate up to 10 viewers (Fig. 7). It was where we had most of our diagnostic and scientific discussions, in particular when we welcomed distinguished visitors such as John J. Kepes (Fig. 7) or Bob D. Terry (Fig. 8). And it was always fun and a pleasure, as well as a place where to preserve the good working atmosphere.
Fig. 7. Daily microscoping sessions were always held around the multi-head viewing microscope, here in the second half of the 1990s when an old and cherished friend and neuropathological giant, John Kepes with wife (in foreground) was visiting from Kansas City. Sitting behind them, Haberler at left and Budka at right, standing from left, Hainfellner, Hussun (a pathologist from Yemen), Jarius, Wanschitz. John had briefly stayed at the NI after the failed Hungarian revolution of 1956.
Fig. 8. Bob Terry, another giant of neuropathology, with the author at an Alzheimer conference in Southern Styria, a wine-growing region, Nov. 2007. Kurt Jellinger in the centre at back. In the early 2000s, a young clinical neurologist arrived from Budapest, Gabor G. Kovacs, to learn some neuropathology. His boss at Semmelweis University, Prof. Szirmai who had stayed as postdoc at the NI two decades before, was reluctant to let him go. Soon I found out why: Gabor became the very best trainee I ever had, with an unbelievable eye for morphology, a sound biological understanding and intelligent translation of neuropathological features into clinical significance, extreme diligence and last but not least, in agreement with Albert Einstein’s dictum that it is character that makes the scientist excellent, an open, warm-hearted nature that made him soon everybody’s darling at the institute. It was Gabor who soon covered most of the research work, most prominently in the prion field but also elsewhere in his broad interests. It is sad for me to realise that he left – in my belief was forced to leave because of the circumstances – two years ago to become full professor in Toronto, Canada, a brain-drain consequence of the turmoils suffered by the institute in recent years, but definitely a deserved recognition for this fine man and scientist. In the years of my directorship, I was indeed lucky to have an excellent staff that was about equally balanced between neuropathology and neurochemistry (Fig. 9). Around the same time when Gabor arrived, Ellen Gelpi, another young researcher, joined from Barcelona. With her warm-hearted Mediterranean-style approach to all matters, irrespective of how important or not they were, she soon became an indispensable hand in diagnosis and research, from prion diseases to tick-borne encephalitis. We lost her for some years to an attractive position as head of a Brain Bank in her home city, but fortunately she is now back and remains the very soul of the institute. Another indispensable mind and soul is Romana Höftberger who trained with Hans Lassmann in neuroimmunology in Vienna, and with Josep Dalmau and Francesc Graus in Barcelona. She has high reputation in research on antibody-mediated disorders of the CNS, actually relevant for both neuropathology and neurochemistry, and thus is now the no-longer-missing-link between the two major areas of work in the institute. Last but not least, Christine Haberler has made her name known in the field of paediatric tumour neuropathology, something that needs very specialised expertise. For me, aging as an “old white man”, it was a pleasure to see a highly successful female touch in achieving the most recent accomplishments of the institute.
Fig. 9. The KIN staff in 2006. 1st row, from left: Hainfellner, Regelsberger, Budka, Ströbel, Gelpi, Pipp, Haberler, Höftberger, Bernheimer, Trabattoni, Preusser; behind, the dedicated laboratory and secretariat staff committed to the success of the institute. With increasing age, and success of KIN in general, I was awarded some prizes that recognised our work in some specific areas. Already as far back as 1982, I had received the Moore Award for the best paper on clinico-pathological correlation at the American Association of Neuropathologists (AANP) meeting; it was for my work on IHC in PML, and I was proud of it because I received the award despite the session chairman’s attempts to disturb my presentation. He insisted to limit the number of slides at my talk; so this was a very distinguished virologist who arbitrarily decided that a youngster had two slides too many than what he personally considered appropriate. No, Sir, I explained politely but firmly to him that I would definitely show all my slides, that numbers of slides don’t matter as long the allotted time frame is kept, but that he could, of course, stop me if I would go overtime. So good arguments do help youngsters against forceful professors. For explanation of the then highly publicised BSE and prion situation, I frequently gave scientific statements to the public by press, TV and radio. These were obviously well received, as I was awarded with the title of “Austrian Scientist of the year 1998”; the prize included also the naming of a star after the awardee in one of the far corners of the universe. In 2004 I received an honorary doctorate from the Medical Academy Łodz in Poland, and in 2008 I had the honour to give the Dorothy Russell Memorial Lecture at the British Neuropathological Society Meeting in London (Fig. 10).
Fig. 10. Lecture at the award ceremony to receive the Dorothy S. Russel Prize by the British Society of Neuropathology in London 2008, in front of a memorizing image of my all-time hero, Lucien J. Rubinstein (photo courtesy of BNS). In 2007, we celebrated the 125th anniversary of the Institute by a dedicated symposium [32]. Many friends, including some from overseas, came to follow a series of lectures and posters on NI/KIN’s history and our more recent achievements. It appeared then that the future of KIN was safe and expected to prosper, and I even speculated whether I would live to see the Institute’s 150th anniversary in 2032. One of my concerns was to maintain and foster a good relation to the non-medical and non-scientific world that is funding everything we do. One possibility was the Children’s University when kids who visited KIN were told about our work and, most importantly, even could touch a human brain if they dared to (Fig. 11).
Fig. 11. Since about 2010, KIN participated in the “Children’s University” with demonstrations of brain anatomy to primary schoolchildren. All are exited to see a real brain – some even do not dare to look. I met my second wife Ivana in 2003 by chance, during a summer most Europeans probably remember, as it was extremely hot and beautiful. After my divorce I used weekends and holidays to make long trips by bike (or by car when it was too hot) and stop in between for a refreshing swim, once even in the big Danube river when a most beautiful young lady caught my eyes. I was immediately hooked. She is Czech, worked as a nurse in mobile care in an area northwest of Vienna, and then took a dip in between like I did. She soon decided to take a job offer in a big municipal hospital in the post-surgery recovery room according to her training in anaesthesia. Our daughter Natalia was born in 2007, and this time circumstances were much more family-friendly than with my earlier family. I had more time to spend with the family, of course never enough in a job such as mine, and it was – and is – an absolute delight to see Natalia growing up. When I went to work in Zurich, Ivana wanted to accompany me with Natalia, but I was unsure how it would work out in a completely different setting, with a foreseeable deadline and much higher costs for schooling and living than in Vienna. So we arranged that the family would stay in Vienna, and in the “guest-worker” tradition of Europe I would live over the week in Switzerland, with commuting flights every Friday afternoon to Vienna, and early Monday morning from Vienna. After I came back from Zurich at the end of 2016, I had of course plenty of time to spend with the family. Ivana was ambitious to do a master’s study of three years and is now a recognised specialist for pain nursing. Two years ago we gave in to Natalia’s dearest wish, and Gorry joined our family, a female Portuguese water dog, which is admired not only by us, but also by practically everybody we meet when walking her (Fig. 12).
Fig. 12. The family in Dec. 2019 at a dog exhibition when Gorry became Austrian Junior Champion. At an age of 65, I felt too active to do little to nothing after retirement in Vienna, so I looked elsewhere and found an announcement for a position of consultant at the Institute of Neuropathology of the University Hospital Zurich, headed by Prof. Adriano Aguzzi. I knew Adriano from several meetings, as he is a renowned prion researcher. Adriano was delighted when I phoned him, and we quickly agreed on my start in Zurich from May 2012. I commuted between Vienna and Zurich by flights on Mondays and Fridays, almost always with the same bunch of expats in the plane. I tried a few times to drive by car, but it is some 750 km and more than 7 hours driving time, a rather exhausting adventure. I lived for my first two years in a hostel tower for university visitors, students and postdocs, high enough to have a spectacular panoramic view of the city, before renting a small apartment near the Limmat river. It was wonderful to walk every morning from there alongside the river to the hospital and back in the evening, watching a lot of waterbirds like cranes, encountering youngsters jumping into the water or balancing on slacklines, and passing by still existing public river baths made entirely of wood, cherished by the locals as “Badis”. In comparison with Vienna, Zurich has a well preserved medieval centre, but is much smaller, much is within walking or biking distance (Adriano turned out to be a passionate mountain biker daily climbing up the Ütliberg overlooking the city), the river is in the very centre, and the lakeside part of town has an almost Mediterranean feeling. So it is a gorgeous place to live indeed. I must admit that I came to Switzerland with some trepidation, as I was unsure how the relation with Adriano, who was well known as strong personality, would work out. In fact, it turned out to be an extremely pleasant and convenient situation: since an eternity, I had suddenly no or few administrative duties but could concentrate on what I like most (and probably do best), studying and diagnosing interesting neuropathological cases. As Adriano was busy with his big experimental lab that comprised some 30-plus postdocs and graduate students in addition to a basic staff of researchers and technicians, he was happy to leave the clinical diagnostic service to me and Elisabeth Rushing, a very friendly and easygoing colleague and most experienced neuropathologist with whom it was a delight to harmoniously share supervision of a young team of motivated and gifted trainees. Elisabeth had specialised in tumour and muscle neuropathology and had been the last head of neuropathology at the legendary Armed Forces Institute of Pathology (AFIP) in Washington, DC, before its closure in 2011. Together with Adriano, I was also responsible for the Swiss National Reference Centre for Human Prion Diseases (NRPE). Overall, my time in Zurich was the very best indeed that could happen to an aging guy at the end of his career. I am most grateful to Adriano – who might have had also some trepidation at start, as I have been considered by some as strong personality as well – to have given me such an opportunity. I learnt a lot there, most notably in experimental neuropathology where I had little experience, but also how to organise and run a successful institute in a way differing from what I was used to do. In fact, after passing the age of 70, it was with a heavy heart that I had to stop my stint in Zurich. For a long time, I thought that formal retirement in Vienna, due for Oct 1st, 2011 (Fig. 13), was still a long shot in the future. Big error, it came quicker than I had imagined. I had made some plans that would be options for that remote time, but in fact, believe it or not, it took me almost by surprise. Somehow lost, I suddenly had to look for attractive possibilities to continue at least some of my activities. So I made a visit as honorary professor to the Naval General Hospital in Beijing, on invitation by Prof. Xiaokun Qi, a neurologist with keen interest in neuropathology. In addition, I visited the Brain Bank, Karolinska Institutet, Huddinge Hospital, Stockholm, Sweden, as Guest Consultant for several times, on invitation by Prof. Bengt Winblad, Caroline Graff and Inger Nennesmo, the local neuropathologist.
Fig. 13. Commemorating plaque given to me by the KIN personnel at my farewell party in 2011. It is in the style of a shop sign in the Habsburg tradition. Its text means “Highly laudable neuropathologist in non-retirement”. However, I hoped most to be able to contribute in some function for KIN in the future. For a few months I was given a room that was soon converted into a secretariat, and I could keep only a desk elsewhere that, again, was taken away after a short time. After these disappointments, I looked for something else and found the position in Zurich described above. After coming back to Vienna from 2017, I continued to work on a few forensic cases every year, giving detailed reports to state attorneys and courts, a good possibility to keep active and in touch with neuropathology. Of course the number of my publications has dwindled down, and at the end of my scientific career I came back to my neuropathological love affair, viruses: most recently, I wrote a chapter on flaviviruses and tick-borne encephalitis (TBE) in an ISN-sponsored book on infections of the nervous system [33]. In view of the present unique global challenge by SARS-CoV2, I hope to be able still to contribute my experience with neuroviral pathology to research on CoVID-19. With regard to the future of KIN, I expected that a search committee would be appointed soon after my retirement by the Rector and Senate of the Medical University Vienna, to fill the vacant position of full Professor of Neuropathology and Institute Director. Such a committee is common practice in most if not all universities when a professor retires, and its aim is to find the best candidate; my personal favourite was Gabor, of course. For unclear reasons – at least for me – this did not happen, and year by year went by while I was in Zurich. My former deputy, Hans Hainfellner, was keen to head the institute but remained formally only deputy director until 2019 when, till the end of that year, the Director of the Institute of Pathology was intermittently appointed to head KIN. Reasons to appoint an external Director were, as I was told, financial frictions between the Medical University Vienna (MUV) and AKH about charging for KIN diagnostic services; in a hybrid fashion, KIN has been funded by both MUV and AKH. Finally and sadly, it was decided to formally degrade the traditionally independent institute on Jan. 1st, 2020, after a highly successful history of 137 years, to a Division of Neuropathology and Neurochemistry of the Neurological Clinic, as a MUV-only organisational unit. This was only the second best option to avoid the worst, i.e. complete disbanding when neuropathology would become part of pathology, and neurochemistry would be incorporated into laboratory medicine. Why the by far very best option was not pursued, i.e. the further existence of such a renowned and successful institution, has remained a mystery, not only for me, but also for other MUV professors. Fortunately Romana Höftberger, an associate professor of KIN with excellent knowledge of both neuropathology and neurochemistry, was made head of the new Division; I am sure she will do her best to steer it into calm waters. Similarly, Prof. Thomas Berger, the Director of the Neurological Clinic and now responsible for the old institute becoming new Division, promises to keep it alive as much as possible. At the end, it is time to balance. Was all indeed as positive as these reflections appear, or is it just due to an extended version of the reminiscence bump? For my professional and family lives, there is definitely nothing to regret. With regard to the role of my beloved neuropathology, I cannot find a better summary definition than what Lucien Rubinstein wrote: “It is that neuropathology is an exquisitely enjoyable pursuit”. The only bitter pill, however, is my personal finale – I never dreamed of becoming the very last director of the original institution that has shaped my whole life. What about the future? For a long time, I used to give a special farewell gift to postdocs and graduate students who trained with me, Santiago Ramón y Cajal’s “Advice to a Young Investigator”. It is an interesting and amusing reading, not only because he was one of the most eminent neuroscientists in history, but also because his advice penetrates virtually every relevant issue of life. A hilarious example is Cajal’s criteria for selecting the best wife for a scientist: she should be unattractive, because otherwise she would be too distractive, and she should be rich, to make the husband financially independent in his research. I don’t have such down to earth advice (and I did not follow that advice). However, I believe in an attitude that seems to imbibe also Ramón y Cajal’s writing and can be put in a nutshell of three words: competence, solidarity and trust. Then, now and forever, they are as essential for a scientist or medical practitioner as for any individual’s life. Still more, they are pivotal in the fight against crises, including what we are now enduring. If we respect and follow them, there is no reason to await the future with trepidation. 1. Budka H: Morphologische Aspekte zerebrovaskulärer Erkrankungen. In: Die zerebrale Apoplexie, Hrsg. G. S. Barolin, pp. 62-79. Stuttgart : Enke 1980 (1. Auflage, 2. Auflage 1983, 3. Auflage 1985). 2. Budka H: Pathology of encephalopathies induced by treatment or prophylaxis of neoplastic lesions of the nervous system. In: Treatment of neoplastic lesions of the nervous system. J. Hildebrand, D. Gangji, eds. (Europ. J. Cancer clin. Oncol. Suppl. 3) pp. 45-50. Pergamon Press, Oxford-New York 1982. 3. Budka H: Brain pathology in the collagen vascular diseases. Angiology 32: 365-372 (1981). 4. Budka H, Sluga E, Heiss W-D: Spastic paraplegia associated with Addison's disease: adult variant of adreno-leukodystrophy. J. Neurol. 213: 237-250 (1976) 5. Budka H, Popow-Kraupp Th: Immunohistological studies in viral encephalitis. Acta neuropathol. Suppl. VII: 142-144 (1981) 6. Budka H, Popow-Kraupp Th: Rabies and Herpes simplex virus encephalitis. An immunohistological study on site and distribution of viral antigens. Virchows Arch A 390: 353-364 (1981) 7. Budka H, Popow-Kraupp Th: Immunmorphologische Untersuchungen viraler Antigene bei verschiedenen Enzephalitiden. Verh. Dtsch. Ges. Pathol. 65: 181-185 (1981) 8. Budka H: Multinucleated giant cells in brain: A hallmark of the acquired immune deficiency syndrome (AIDS). Acta neuropathol. 69: 253-258 (1986) 9. Kleihues P, Lang W, Burger PC, Budka H, Vogt M, Maurer R, Lüthy R, Siegenthaler W: Progressive diffuse leukoencephalopathy in patients with acquired immune deficiency syndrome (AIDS). Acta neuropathol. 68: 333-339 (1985) 10. Budka H, Costanzi G, Cristina S, Lechi A, Parravicini C, Trabattoni R, Vago L: Brain pathology induced by infection with the human immunodeficiency virus (HIV). A histological, immunocytochemical, and electron microscopical study of 100 autopsy cases. Acta neuropathol. 75: 185-198 (1987) 11. Budka H: Human immunodeficiency virus (HIV) envelope and core proteins in CNS tissues of patients with the acquired immune deficiency syndrome (AIDS). Acta neuropathol 79: 611-619 (1990) 12. Ketzler S, Weis S, Haug H, Budka H: Loss of neurons in the frontal cortex in AIDS brains. Acta neuropathol 80: 92-94 (1990) 13. Hainfellner JA, Brantner-Inthaler S, Cervenáková L, Brown P, Kitamoto T, Tateishi J, Diringer H, Liberski PP, Regele H, Feucht M, Mayr N, Wessely P, Summer K, Seitelberger F, Budka H: The original Gerstmann-Sträussler-Scheinker family of Austria: divergent clinicopathological phenotypes but constant PrP genotype. Brain Pathol 5: 201-211 (1995) 14. Kretzschmar HA, Honold G, Seitelberger F, Feucht M, Wessely P, Mehraein P, Budka H: Prion protein mutation in family first reported by Gerstmann, Sträussler, and Scheinker. Lancet 337: 1160 (1991) 15. Vossen P, Kreysa J, Goll M (eds): Overview of the BSE risk assessments of the European Commission’s Scientific Steering Committee (SSC) and its TSE/BSE ad hoc Group adopted between September 1997 and April 2003. pp. 18-34. European Commission, published online June 5, 2003; https://ec.europa.eu/food/sites/food/files/safety/docs/sci-com_ssc_out364_en.pdf 16. Budka H, Will RG: The end of the BSE saga: do we still need surveillance for human prion diseases? Swiss Med Wkly 145:w14212 (2015) 17. Kosaka K., M. Yoshimura, K. Ikeda, H. Budka: Diffuse type of Lewy body disease: A progressive dementia with numerous cortical Lewy bodies and senile changes of varying degree - A new disease? Clin. Neuropathol. 3: 185-192 (1984) 18. Budka H, Aguzzi A, Brown P, Brucher J-M, Bugiani O, Gullotta F, Haltia M, Hauw J-J, Ironside JW, Jellinger K, Kretzschmar HA, Lantos PL, Masullo C, Schlote W, Tateishi J, Weller RO: Neuropathological diagnostic criteria for Creutzfeldt-Jakob disease (CJD) and other human spongiform encephalopathies (prion diseases). Brain Pathol 5: 459-466 (1995) 19. Budka H: Neuropathology of prion diseases. Brit Med Bull 66: 121-130 & Plate X (2003) 20. Kovács GG, Preusser M, Strohschneider M, Budka H: Subcellular localization of disease associated prion protein in the human brain. Am J Pathol 166: 287-294 (2005) 21. Makarava N, Kovacs GG, Bocharova O, Savtchenko R, Alexeeva I, Budka H, Rohwer RG, Baskakov IV: Recombinant prion protein induces a new transmissible prion disease in wild type animals. Acta Neuropathol 119/2: 177-187 (2010) 22. Budka H: Neuropathology of human immunodeficiency virus infection. Brain Pathol 1: 163-175 (1991) 23. Gelpi E, Preusser M, Garzuly F, Holzmann H, Heinz FX, Budka H: Visualization of Central European tick borne encephalitis infection in fatal human cases. J Neuropathol Exp Neurol 64: 506-512 (2005) 24. Herpers MJHM, Budka H: Glial fibrillary acidic protein (GFAP) in oligodendroglial tumors: gliofibrillary oligodendroglioma and transitional oligoastrocytoma as subtypes of oligodendroglioma. Acta neuropathol. 64: 265-272 (1984) 25. Maier H, Öfner D, Hittmair A, Kitz K, Budka H: Classical, "atypical" and anaplastic meningioma: three histopathological subtypes of clinical relevance. J Neurosurg 77: 616-623 (1992) 26. Kovacs GG, Majtenyi K, Spina S, Murrell JR, Gelpi E, Hoftberger R, Fraser G, Crowther RA, Goedert M, Budka H, Ghetti B: White matter tauopathy with globular glial inclusions: a distinct entity of sporadic frontotemporal lobar degeneration. J Neuropathol Exp Neurol 67: 963-975 (2008) 27. Kovacs GG, Milenkovic IJ, Preusser M, Budka H: Nigral burden of a-synuclein correlates with striatal dopamine deficit. Mov Disord 23 (11): 1608-1612 (2008) 28. Kovacs GG, Breydo L, Green R, Kis V, Puska G, Lőrincz P, Perju-Dumbrava L, Giera R, Pirker W, Lutz M, Lachmann I, Budka H, Uversky VN, Molnár K, László L: Intracellular processing of disease-associated α-synuclein in the human brain suggests prion-like cell-to-cell spread. Neurobiol Dis 69: 76-92 (2014) 29. Kovacs GG, Botond G, Budka H: Protein coding of neurodegenerative dementias: the neuropathological basis of biomarker diagnostics. Acta Neuropathol 119: 389-408 (2010) 30. Kovacs GG, Milenkovic I, Wöhrer A, Höftberger R, Gelpi E, Haberler C, Hönigschnabl S, Reiner-Concin A, Heinzl H, Jungwirth S, Krampla W, Fischer P, Budka H: Non-Alzheimer neurodegenerative pathologies and their combinations are more frequent than commonly believed in the elderly brain: a community-based autopsy series. Acta Neuropathol 126: 365-384 (2013) 31. Frontzek K, Lutz MI, Aguzzi A, Kovacs GG, Budka H: Amyloid-β pathology and cerebral amyloid angiopathy are frequent in iatrogenic Creutzfeldt-Jakob disease after dural grafting. Swiss Med Wkly 146:w14287 (2016) 32. Kreft G, Kovacs GG, Voigtländer T, Haberler C, Hainfellner JA, Bernheimer H, Budka H: 125th anniversary of the Institute of Neurology (Obersteiner Institute) in Vienna. “Germ Cell” of Interdisciplinary Neuroscience. Clin Neuropathol 27: 439-443 (2008) 33. Budka H: Flaviviruses 1. General Introduction and Tick Borne Encephalitis. In: Chrétien F, Wong KT, Sharer LR, Keohane C, Gray F (eds) Infections of the Central Nervous System: Neuropathology and Genetics. International Society of Neuropathology (ISN) Book Series Pathology and Genetics, Chapter 14, pp 131-146. Wiley, Hoboken, NJ 2020 List of neuropathological research visitors and postdocs who trained in neuropathology in the NI/KIN: Masanori Tomonaga, Professor in Tokyo, Riki Okeda, Professor in Tokyo, Takeshi Kurata, Professor at the NIH Tokyo, Ichiro Akiguchi, Professor in Kyoto, Toshihiko Suenaga, Yoshitomo Shirakashi, Yasuhiro Kawamoto, Hiroshi Sugiyama, Toru Kimura, Kyoko Ozawa, all Kyoto, Masahiro Yoshimura-Yasuhara, Hitoshi Yamanouchi, both Tokyo, Noburo Kochi, Tatsuo Morimura, both Hyogo, Kazuko Sato-Matsumura, Sapporo, Sami Khoshyomn, Burlington VT, Silvia Cristina, Milano, Gianriccardo Trabattoni, Parma, Carlos Lima, Lisboa, Mara Popovic, Professor in Ljubljana, Raf Sciot, Louvain, Marcel JHM Herpers, Professor in Maastricht, Ferenc Garzuly, Szombathely, Tibor Hortobágyi, Professor in Szeged, Felicia Slowik, Budapest, Andras Guseo, Székesfehérvár, Pawel P. Liberski, Professor in Łodz, Beata Sikorska, Professor in Łodz, Radek Kordek, Łodz, Maria Barcikowska, Łodz, Radek Matej, Professor in Prague, Marin Guentchev, Professor in Sofia, Ognan Kalev, Sofia, later Linz, Yervand Karapetyan, Armenia, Hussun, Yemen, Sashine Tolunay, Bursa, Karl Rössler, Professor in Vienna, Christian Bancher, Horn, Eduard Auff, Professor in Vienna, Stefan Klöppel, Professor in Freiburg i. Br, Peter Pilz, Salzburg, Hans Maier, Innsbruck, Christine Wüstinger, Johannes Preiser, Elisabeth Wondrusch, Claudia Radbauer, Peter Mazal, Oskar Koperek, Christa Jarius, Elisabeth Lindeck-Pozza, Anna C Rudnay, Roland Sedivy, Ute Laggner, Irene Pipp, Ivan J Milenkovic, Harald Stefanits, all Vienna, Michael Huemer, Schwarzach-St. Veit, Reza Yassari, Chicago IL. I apologise to those whom I missed, as I could not cross-check the list with documents in the institute. Past and present neuropathological researchers who have worked for prolonged periods in the NI/KIN include Ellen Gelpi, Johannes Hainfellner, Christine Haberler, Romana Höftberger, Gabor G. Kovacs, Matthias Preusser, Manfred Schmidbauer, Sabine Urbanits, Julia Wanschitz, Adelheid Wöhrer.
Copyright: © 2020 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |